

Volume 6, Issue 4 (11-2019)
JROS 2019, 6(4): 25-30 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Valiollahi B, Salehpour M, Bashari H, Majdi S, Mohammadpour M. A Typical Metatarsal Fracture in a Patient on Long-Term Bisphosphonate Therapy. JROS 2019; 6 (4) :25-30
URL: http://jros.iums.ac.ir/article-1-2043-en.html
URL: http://jros.iums.ac.ir/article-1-2043-en.html



1- Bone and Joint Reconstruction Research Center, Shafa Orthopedic Hospital, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 1862 kb]
(983 Downloads)
| Abstract (HTML) (1828 Views)
Full-Text: (1601 Views)
1. Introduction
Stress fractures occur as a result of repetitive loading and unloading of a bone [1]. Increased strain or frequency of compression and tension loads may lead to microfractures, which are repaired during the bone remodeling process. A stress fracture may develop when extensive microdamage exceeds the bone remodeling process [2, 3]. Although these fractures are mostly observed in lower limb bones of runners, dancers, and military personnel, they may also arise in individuals with rheumatoid arthritis and metabolic bone diseases [4, 5]. Additionally, drugs such as bisphosphonates contribute to developing bone fractures.
Bisphosphonates are preferred drugs in postmenopausal and corticosteroid-induced osteoporosis [6]. Patients under long-term treatment by bisphosphonates usually experience subtrochanteric and femoral shaft fractures. Though there are limited reports regarding pathological fractures at other musculoskeletal sites [7, 8]. the present study presents a rare case of alendronate-induced pathological metatarsal fracture.
2. Case Presentation
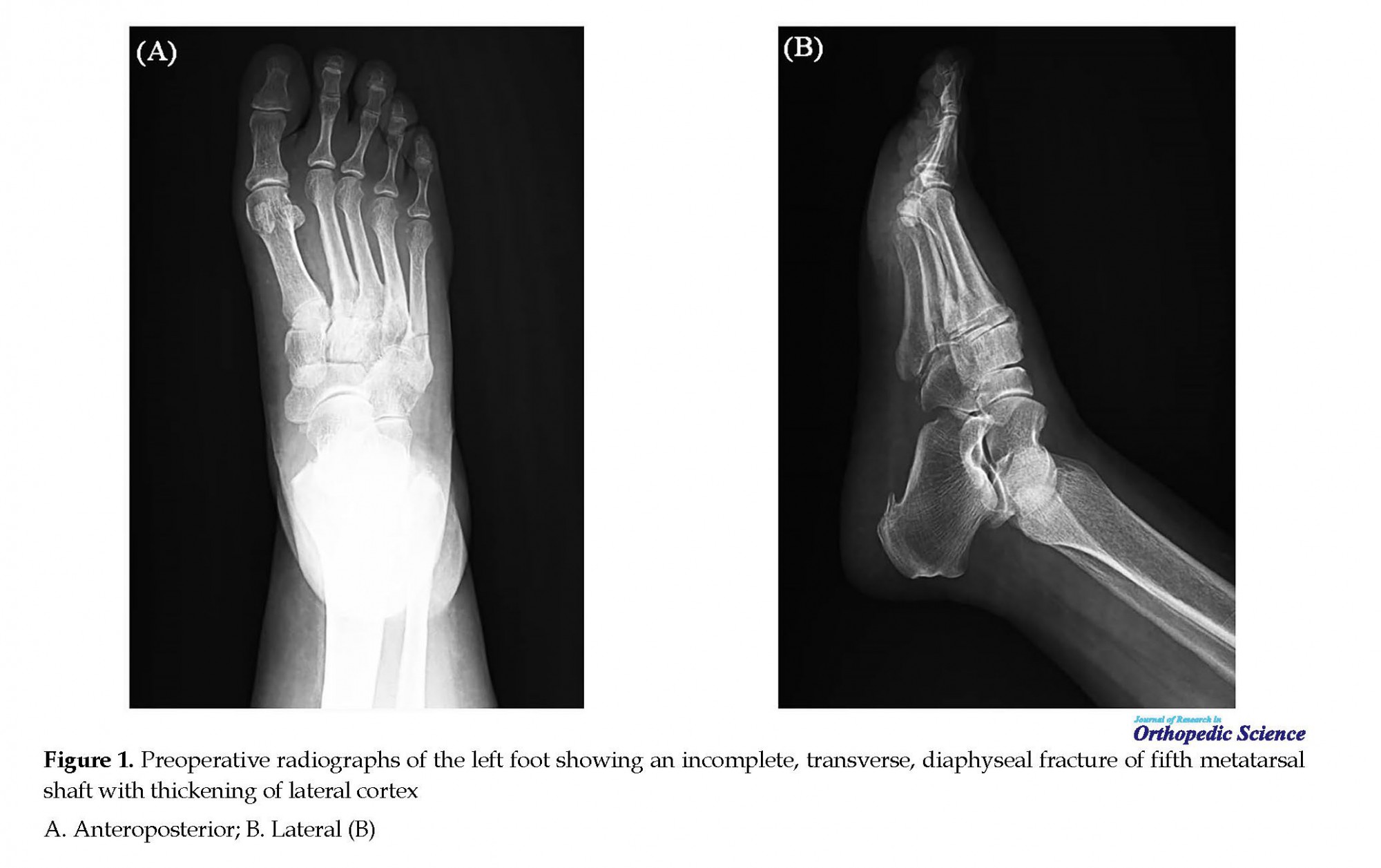
A 59-year-old female presented with a history of cuboid fracture following a twisting in 2013 with abnormal Bone Mineral Density (BMD) (T score: −3.5; lumbar spine and −2.6; proximal femur), suggesting severe osteoporosis. Thus, she was advised to take alendronate 70 mg once a week with calcium supplementation. After 2 years, a dull pain started in the left foot insidiously, which did not subside with conservative treatments such as analgesics consumption for 5 months and splint for 6 weeks. The radiographic evaluations showed an incomplete, transverse, diaphyseal fracture of the fifth metatarsal shaft along with the thickening of the lateral cortex (Figure 1).
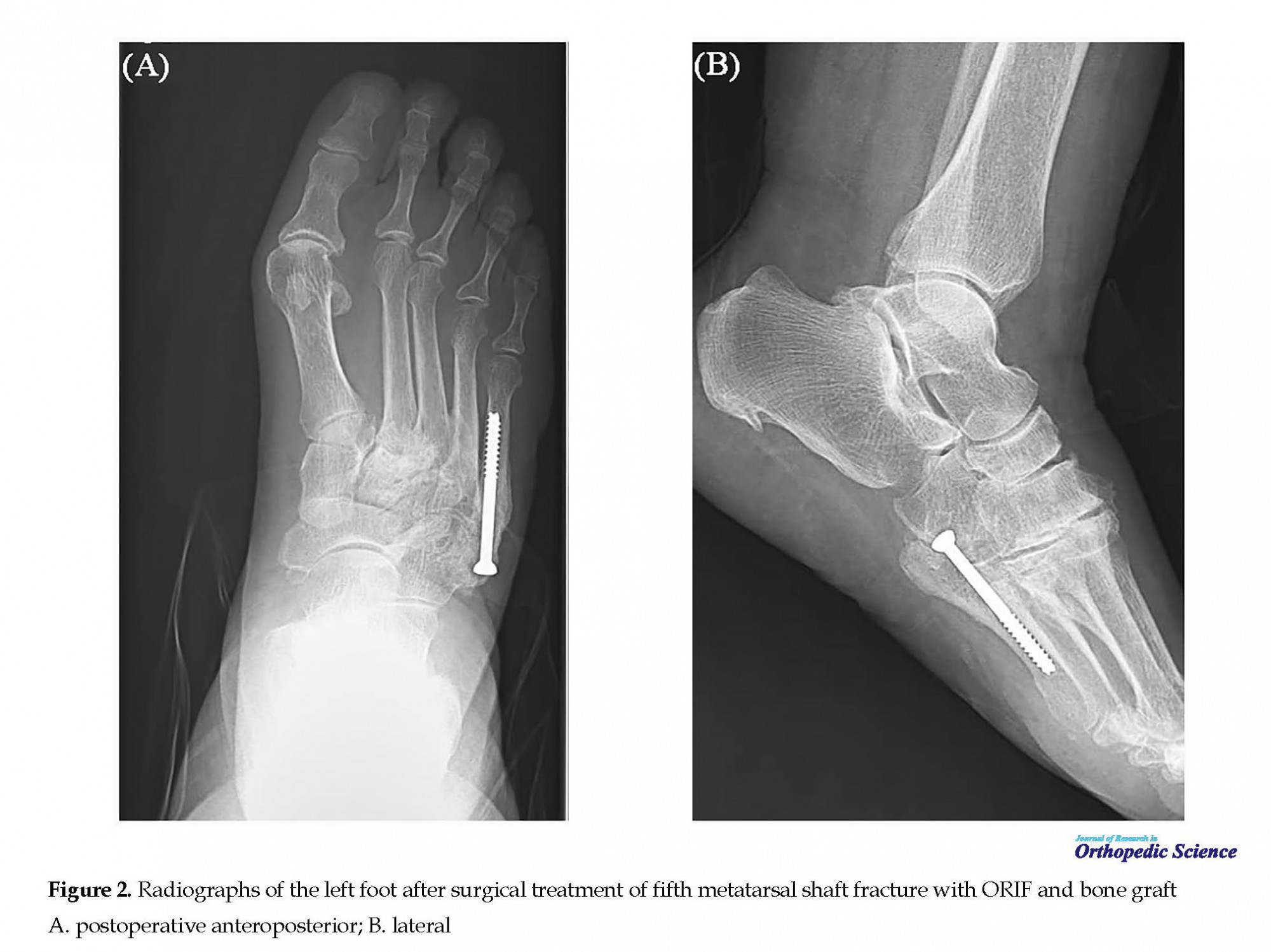
The patient’s BMD result indicated osteopenia (T score: -1.2). Also, the whole body bone scan revealed a stress fracture in the left fifth metatarsal bone. Accordingly, the patient underwent an operation. In operation, open reduction, internal fixation, bone graft, and biopsy were performed (Figure 2). The results of the biopsy showed the reactive bone formation and Severely Suppression of Bone Turnover (SSBT). Therefore, alendronate therapy was discontinued, and subcutaneous teriparatide 20 µg therapy started and continued for 6 months. In the follow-up, the symptoms improved and the fracture healed. After 3 months, the patient returned to her household routine and could walk without walking aid.
3. Discussion
Bisphosphonates are the most widely studied and first-line category of drugs for the treatment of postmenopausal and corticosteroid-induced osteoporosis [9]. In this category, the Food and Drug Administration has approved alendronate for the treatment for osteoporosis [10]. Bisphosphonates mainly bind to mineralized bone surfaces and reduce osteoclastic bone resorption and result in an increased mineral density noticeable in dual-energy X-ray absorptiometry scans [6]. Paradoxically, this dense bone is weaker, more brittle, and more prone to pathological fractures. Alendronate significantly increases the bone density of the spine and hip and reduces the incidence of osteoporotic fracture up to 50% [11]. Even when discontinued after 5 years, the physiological effect on bone resorption remains for 5 years after that with no increase in fracture risk [11].
Stress fractures occur as a result of repetitive loading and unloading of a bone [1]. Increased strain or frequency of compression and tension loads may lead to microfractures, which are repaired during the bone remodeling process. A stress fracture may develop when extensive microdamage exceeds the bone remodeling process [2, 3]. Although these fractures are mostly observed in lower limb bones of runners, dancers, and military personnel, they may also arise in individuals with rheumatoid arthritis and metabolic bone diseases [4, 5]. Additionally, drugs such as bisphosphonates contribute to developing bone fractures.
Bisphosphonates are preferred drugs in postmenopausal and corticosteroid-induced osteoporosis [6]. Patients under long-term treatment by bisphosphonates usually experience subtrochanteric and femoral shaft fractures. Though there are limited reports regarding pathological fractures at other musculoskeletal sites [7, 8]. the present study presents a rare case of alendronate-induced pathological metatarsal fracture.
2. Case Presentation
A 59-year-old female presented with a history of cuboid fracture following a twisting in 2013 with abnormal Bone Mineral Density (BMD) (T score: −3.5; lumbar spine and −2.6; proximal femur), suggesting severe osteoporosis. Thus, she was advised to take alendronate 70 mg once a week with calcium supplementation. After 2 years, a dull pain started in the left foot insidiously, which did not subside with conservative treatments such as analgesics consumption for 5 months and splint for 6 weeks. The radiographic evaluations showed an incomplete, transverse, diaphyseal fracture of the fifth metatarsal shaft along with the thickening of the lateral cortex (Figure 1).
The patient’s BMD result indicated osteopenia (T score: -1.2). Also, the whole body bone scan revealed a stress fracture in the left fifth metatarsal bone. Accordingly, the patient underwent an operation. In operation, open reduction, internal fixation, bone graft, and biopsy were performed (Figure 2). The results of the biopsy showed the reactive bone formation and Severely Suppression of Bone Turnover (SSBT). Therefore, alendronate therapy was discontinued, and subcutaneous teriparatide 20 µg therapy started and continued for 6 months. In the follow-up, the symptoms improved and the fracture healed. After 3 months, the patient returned to her household routine and could walk without walking aid.
3. Discussion
Bisphosphonates are the most widely studied and first-line category of drugs for the treatment of postmenopausal and corticosteroid-induced osteoporosis [9]. In this category, the Food and Drug Administration has approved alendronate for the treatment for osteoporosis [10]. Bisphosphonates mainly bind to mineralized bone surfaces and reduce osteoclastic bone resorption and result in an increased mineral density noticeable in dual-energy X-ray absorptiometry scans [6]. Paradoxically, this dense bone is weaker, more brittle, and more prone to pathological fractures. Alendronate significantly increases the bone density of the spine and hip and reduces the incidence of osteoporotic fracture up to 50% [11]. Even when discontinued after 5 years, the physiological effect on bone resorption remains for 5 years after that with no increase in fracture risk [11].
It is believed that subtrochanteric stress fractures, pelvic insufficiency fractures, and femoral fractures are associated with the long-term consumption of bisphosphonate [12]. In this regard, metatarsal stress fractures have been observed, as well [13, 14]. In 2005, Odvina et al. identified a group of 9 patients who developed spontaneous non-spinal fractures while on the long-term consumption of alendronate. These non-traumatic fractures affect skeletal areas rich in cortical bone, such as the femoral shaft, pubic bone, and ischium that was atypical for osteoporotic fractures. Notably, bone biopsies demonstrated SSBT in all cases [15].
It has been reported that the long-term consumption of alendronate, especially in patients with normal BMD, leads to SSBT, resulting in bone pains and pathological fractures [8, 10]. Based on experimental studies, alendronate can inhibit the natural process of repairing microdamages arising from SSBT, which in turn results in the accumulation of microdamage. In addition to microdamage accumulation, chronic over-SSBT by alendronate may allow secondary mineralization to continue, resulting in the hyper-mineralized bone. Primarily, a hyper-mineralized bone has a higher Young’s modulus, but a lower work to failure (a measure of fracture toughness) [16].
It has been reported that the long-term consumption of alendronate, especially in patients with normal BMD, leads to SSBT, resulting in bone pains and pathological fractures [8, 10]. Based on experimental studies, alendronate can inhibit the natural process of repairing microdamages arising from SSBT, which in turn results in the accumulation of microdamage. In addition to microdamage accumulation, chronic over-SSBT by alendronate may allow secondary mineralization to continue, resulting in the hyper-mineralized bone. Primarily, a hyper-mineralized bone has a higher Young’s modulus, but a lower work to failure (a measure of fracture toughness) [16].
Alendronate-associated fractures may be bilateral and have unique radiological features such as transverse fracture orientation with pre-existing ellipsoidal thickening of lateral femoral cortex and medial beak [8]. They are likely to be preceded by prodromal pain and occur with or without trivial trauma. These fractures are mainly reported in the subtrochanteric and diaphyseal region of the femur; however, a long-term alendronate therapy in the present case may be a contributing factor in concomitant pathological fractures at other musculoskeletal sites.
In this case, a patient with limited function in daily activities and a history of bone fracture in the past was on long-term alendronate therapy for 2 years. She had an ordinary bone stock with a near-normal BMD (T score: -1.2). Nevertheless, the fracture occurred in the fifth metatarsal bone along with preceding prodromal symptoms and without the history of trauma. Moreover, the characteristic features included incomplete transverse diaphyseal fractures with the thickening of the lateral cortex at the fifth metatarsal.
These fractures are substantially difficult to heal with conservative management [17]. The currently-accepted guideline for the treatment of incomplete or complete fractures is operation along with discontinuation of bisphosphonate therapy and the introduction of subcutaneous low-dose teriparatide 20 µg every day for 3 to 6 months. In this case, there was a remarkable improvement in BMD after long-term alendronate therapy. However, since in some patients, this prolonged treatment may contribute to SSBT, it does not seem to be a safe treatment [17].
There are serious concerns about the long-term use of alendronate, which may lead to SSBT and unusual fractures. The recognition of this fracture pattern among patients, who are on long-term monthly Nitrogen containing Bisphosphonates therapy (N-BP's), will hopefully encourage additional studies that address the etiology of these fractures and potential therapeutic maneuvers that can reduce their occurrence and improve patient outcomes.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Designing the study: Bijan Valiollahi, Mostafa Salehpour; Data collection and analysis: Mehdi Mohammadpour, Shoeib Majdi; Writing the manuscript: Mostafa Salehpour, Hamidreza Bashari; Reviewing – Editing the manuscript: Mehdi Mohammadpour, Mostafa Salehpour; Supervision: Mostafa Salehpour.
Conflict of interest
The authors declared no conflict of interest.
References
Maitra RS, Johnson DL. Stress fractures, clinical history and physical examination. Clin Sports Med. 1997; 16(1):259-74. [DOI:10.1016/S0278-5919(05)70021-1]
Arndt A, Ekenman I, Westblad P, Lundberg A. Effects of fatigue and load variation on metatarsal deformation measured in vivo during barefoot walking. J Biomech. 2002; 35(1):621-8. [DOI:10.1016/S0021-9290(01)00241-X]
Uthgenannt BA, Kramer MH, Hwu JA, Wopenka B, Silva MJ. Skeletal self-repair: Stress fracture healing by rapid formation and densification of woven bone. J Bone Miner Res. 2007; 22(2):1548-56 [DOI:10.1359/jbmr.0070614] [PMID] [PMCID]
Smrcina CM. Stress fractures in athletes. Nurs Clin North Am. 1991; 26(2):159-66.
Hockenbury RT. Forefoot problems in athletes. Med Sci Sports Exerc. 1999; 31(suppl. 7):S448-58. [DOI:10.1097/00005768-199907001-00006] [PMID]
Russell RG, Croucher PI, Rogers MJ. Bisphosphonates: Pharmacology, mechanisms of action and clinical uses. Osteoporosis Int. 1999; 9(suppl. 2):S66-80. [DOI:10.1007/PL00004164] [PMID]
Imai K, Yamamoto S, Anamizu Y, Horiuchi T. Pelvic insufficiency fracture associated with severe suppression of bone turnover by alendronate therapy. J Bone Miner Metab. 2007; 25(5):333-6. [DOI:10.1007/s00774-007-0771-y] [PMID]
Chan SS, Rosenberg ZS, Chan K, Capeci C. Subtrochanteric femoral fractures in patients receiving longterm alendronate therapy: Imaging features. Am J Roentgenol. 2010; 194(2):1581-6. [DOI:10.2214/AJR.09.3588] [PMID]
Drake MT, Clarke BL, Khosala S. Bisphosphonate: Mechanism of action and role in clinical practice. Mayo Clin Proc. 2008; 83(1):1032-45. [DOI:10.4065/83.9.1032] [PMID] [PMCID]
US Food and Drug Administration. FDA Drug Safety Communication: Safety update for osteoporosis drugs, bisphosphonates, and atypical fractures. Silver Spring: US Food and Drug Administration; 2010.
Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing fracture, fracture intervention trial research group. Lancet. 1996; 348(3):1535-41. [DOI:10.1016/S0140-6736(96)07088-2]
Lenart BA, Neviaser AS, Lyman S, Chang CC, Edobor-Osula F, Steele B, et al. Association of low-energy femoral fractures with prolonged bisphosphonate use: A case control study. Osteoporos Int. 2009; 20(8):1353-62. [DOI:10.1007/s00198-008-0805-x] [PMID] [PMCID]
Schneider JP. Should bisphosphonates be continued indefinitely? An unusual fracture in a healthy woman on long-term alendronate. Geriatrics. 2006; 61(1):31-3. [PMID]
Pradhan P, Saxena V, Yadav A, Mehrotra V. Atypical metatarsal fracture in a patient on long term bisphosphonate therapy. Indian J orthop. 2012; 46(5):589-92. [DOI:10.4103/0019-5413.101048] [PMID] [PMCID]
Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: A potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005; 90(2):1294-301. [DOI:10.1210/jc.2004-0952] [PMID]
Mashiba T, Turner CH, Hirano T, Forwood MR, Johnston CC, Burr DB. Effects of suppressed bone turnover by bisphosphonates on microdamage accumulation and biomechanical properties in clinically relevant skeletal sites in beagles. Bone. 2001; 28(3):524-31. [DOI:10.1016/S8756-3282(01)00414-8]
Goh SK, Yang KY, Koh JS, Wong MK, Chua SY, Chua DT, et al. Subtrochanteric insufficiency fractures in patients on alendronate therapy: A caution. J Bone Joint Surg Br. 2007; 89(1):349-53. [DOI:10.1302/0301-620X.89B3.18146] [PMID]
In this case, a patient with limited function in daily activities and a history of bone fracture in the past was on long-term alendronate therapy for 2 years. She had an ordinary bone stock with a near-normal BMD (T score: -1.2). Nevertheless, the fracture occurred in the fifth metatarsal bone along with preceding prodromal symptoms and without the history of trauma. Moreover, the characteristic features included incomplete transverse diaphyseal fractures with the thickening of the lateral cortex at the fifth metatarsal.
These fractures are substantially difficult to heal with conservative management [17]. The currently-accepted guideline for the treatment of incomplete or complete fractures is operation along with discontinuation of bisphosphonate therapy and the introduction of subcutaneous low-dose teriparatide 20 µg every day for 3 to 6 months. In this case, there was a remarkable improvement in BMD after long-term alendronate therapy. However, since in some patients, this prolonged treatment may contribute to SSBT, it does not seem to be a safe treatment [17].
There are serious concerns about the long-term use of alendronate, which may lead to SSBT and unusual fractures. The recognition of this fracture pattern among patients, who are on long-term monthly Nitrogen containing Bisphosphonates therapy (N-BP's), will hopefully encourage additional studies that address the etiology of these fractures and potential therapeutic maneuvers that can reduce their occurrence and improve patient outcomes.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Designing the study: Bijan Valiollahi, Mostafa Salehpour; Data collection and analysis: Mehdi Mohammadpour, Shoeib Majdi; Writing the manuscript: Mostafa Salehpour, Hamidreza Bashari; Reviewing – Editing the manuscript: Mehdi Mohammadpour, Mostafa Salehpour; Supervision: Mostafa Salehpour.
Conflict of interest
The authors declared no conflict of interest.
References
Maitra RS, Johnson DL. Stress fractures, clinical history and physical examination. Clin Sports Med. 1997; 16(1):259-74. [DOI:10.1016/S0278-5919(05)70021-1]
Arndt A, Ekenman I, Westblad P, Lundberg A. Effects of fatigue and load variation on metatarsal deformation measured in vivo during barefoot walking. J Biomech. 2002; 35(1):621-8. [DOI:10.1016/S0021-9290(01)00241-X]
Uthgenannt BA, Kramer MH, Hwu JA, Wopenka B, Silva MJ. Skeletal self-repair: Stress fracture healing by rapid formation and densification of woven bone. J Bone Miner Res. 2007; 22(2):1548-56 [DOI:10.1359/jbmr.0070614] [PMID] [PMCID]
Smrcina CM. Stress fractures in athletes. Nurs Clin North Am. 1991; 26(2):159-66.
Hockenbury RT. Forefoot problems in athletes. Med Sci Sports Exerc. 1999; 31(suppl. 7):S448-58. [DOI:10.1097/00005768-199907001-00006] [PMID]
Russell RG, Croucher PI, Rogers MJ. Bisphosphonates: Pharmacology, mechanisms of action and clinical uses. Osteoporosis Int. 1999; 9(suppl. 2):S66-80. [DOI:10.1007/PL00004164] [PMID]
Imai K, Yamamoto S, Anamizu Y, Horiuchi T. Pelvic insufficiency fracture associated with severe suppression of bone turnover by alendronate therapy. J Bone Miner Metab. 2007; 25(5):333-6. [DOI:10.1007/s00774-007-0771-y] [PMID]
Chan SS, Rosenberg ZS, Chan K, Capeci C. Subtrochanteric femoral fractures in patients receiving longterm alendronate therapy: Imaging features. Am J Roentgenol. 2010; 194(2):1581-6. [DOI:10.2214/AJR.09.3588] [PMID]
Drake MT, Clarke BL, Khosala S. Bisphosphonate: Mechanism of action and role in clinical practice. Mayo Clin Proc. 2008; 83(1):1032-45. [DOI:10.4065/83.9.1032] [PMID] [PMCID]
US Food and Drug Administration. FDA Drug Safety Communication: Safety update for osteoporosis drugs, bisphosphonates, and atypical fractures. Silver Spring: US Food and Drug Administration; 2010.
Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing fracture, fracture intervention trial research group. Lancet. 1996; 348(3):1535-41. [DOI:10.1016/S0140-6736(96)07088-2]
Lenart BA, Neviaser AS, Lyman S, Chang CC, Edobor-Osula F, Steele B, et al. Association of low-energy femoral fractures with prolonged bisphosphonate use: A case control study. Osteoporos Int. 2009; 20(8):1353-62. [DOI:10.1007/s00198-008-0805-x] [PMID] [PMCID]
Schneider JP. Should bisphosphonates be continued indefinitely? An unusual fracture in a healthy woman on long-term alendronate. Geriatrics. 2006; 61(1):31-3. [PMID]
Pradhan P, Saxena V, Yadav A, Mehrotra V. Atypical metatarsal fracture in a patient on long term bisphosphonate therapy. Indian J orthop. 2012; 46(5):589-92. [DOI:10.4103/0019-5413.101048] [PMID] [PMCID]
Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: A potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005; 90(2):1294-301. [DOI:10.1210/jc.2004-0952] [PMID]
Mashiba T, Turner CH, Hirano T, Forwood MR, Johnston CC, Burr DB. Effects of suppressed bone turnover by bisphosphonates on microdamage accumulation and biomechanical properties in clinically relevant skeletal sites in beagles. Bone. 2001; 28(3):524-31. [DOI:10.1016/S8756-3282(01)00414-8]
Goh SK, Yang KY, Koh JS, Wong MK, Chua SY, Chua DT, et al. Subtrochanteric insufficiency fractures in patients on alendronate therapy: A caution. J Bone Joint Surg Br. 2007; 89(1):349-53. [DOI:10.1302/0301-620X.89B3.18146] [PMID]
Type of Study: Case Report |
Subject:
Knee surgery
Received: 2019/05/3 | Accepted: 2019/12/25 | Published: 2019/12/25
Received: 2019/05/3 | Accepted: 2019/12/25 | Published: 2019/12/25
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
