

Volume 7, Issue 2 (5-2020)
JROS 2020, 7(2): 67-72 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Andalib A, Akbari Aghdam H, Ahmadi E. Different Traumatic Spinal Column Fractures and Traumatic Spinal Cord Injury: An Epidemiologic Study. JROS 2020; 7 (2) :67-72
URL: http://jros.iums.ac.ir/article-1-2095-en.html
URL: http://jros.iums.ac.ir/article-1-2095-en.html
Different Traumatic Spinal Column Fractures and Traumatic Spinal Cord Injury: An Epidemiologic Study



1- Department of Orthopedics, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
Full-Text [PDF 583 kb]
(938 Downloads)
| Abstract (HTML) (2272 Views)
Full-Text: (953 Views)
1. Introduction
Trauma is the most common cause ofdisabilities among the young populationin developing countries [1]. Aside from morbidity and mortality, traumaticinjuries can significantly decrease thequality of life and life expectancy of the victims. Traumatic injuries are mostcommon in the younger working population but they arealso high among the older population [2]. Spinal column injuries are rare, but they can cause high mortality andmorbidity rates with heavy burdens and lifelong social, financial, and personal problems and even permanent disabilities [3]. Traumatic spinal column injuries are alsohigh in low socio-economic areas due to frequent use of motorcycles, lack of sufficient immunity, and absence of adequate infrastructures.
Traumatic Spinal Cord Injury (TSCI) can occur afterspinal column injury [4]. TSCI is an acute, traumatic lesion of the spinal cord with its consequent economic problems and can emotionally and psychologically affect the patients. It can affect different systems andorgans of the body and cause motor or sensory impairmentsor dysfunction of urinary, gastrointestinal, or reproductivesystems [5]. TSCI in pediatric or young populationis a catastrophic event that can alter the child’s life forever. Different studies had surveys about the incidence of TSCI around the world and this incidence ranges from 3.6 to 195.4 patients per million around the world [6].
Studies indicate that TSCI is mostly caused by vehicle accidents, falling, and violence. Age distribution for TSCI also showed a higher incidence in 15-29 and over65 years old people [7]. These data indicate the importance of TSCI because it affects mostly younger working population causing heavy socio-economic burden and older population in whom serious complications are observed. TSCI can permanently damage different organs but they may be rehabilitated by the means of physiotherapies or occupational therapies [8]. Evidence shows that early surgical intervention in cases that require immediate surgery could be a great help in further prognosis [9]. Different studies surveyed the epidemiology of TSCI and evaluated age and sex distributions and relatedfactors. This study aims to evaluate spinal column fractures based on anatomical position, percentage of TSCI, and need for surgery in Iran. This information can enrich our knowledge of spinal cord trauma and safety considerations at the scene of the accident.
2. Methods
This is a retrospective study of cases with traumatic spinal column fractures referring to Al-Zahra Hospital, one of the most important trauma centers of Isfahan City, Iran. We evaluated all cases diagnosed with traumaticspinal column fractures between 2012 and 2018. A total of 1014 patients were included in our study. The exclusion criteria were lacking clear spine radiology images or patients with severe brain injury. The study was approved by the Ethics Committee of Isfahan University of Medical Sciences. All medical records of patients were reviewed and anatomical locations of spine fractureswere evaluated. Patients with spinal cord injuries were also detected based on documented history andMRI findings. The need for surgery and the percentage of TSCI were also evaluated. The obtained data wereanalyzed in SPSS.
3. Results
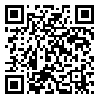
In this study, 1014 patients with traumatic spinal columnfractures were included. The most common causes of trauma were vehicle and road accidents (83.4%) followed by falling (12.7%). Sex distribution indicated that 717 cases (70.7%) were male and 297 (29.3%) female. Furthermore, 7.1% of male patients had spinal injurieswhile only 3.7% of females had spinal injuries and thisdifference was statistically significant (P=0.024). A total of 21 patients (2.1%) died due to injuries. Statistics showed that 85.7% of mortalities occurred in males and 14.3% in females and as a result, male patients with traumatic spine injuries had higher mortalities. The frequencyof TSCI among patients with traumatic spinal column fractures were 62 patients (6.1%). Further analysis also indicated that 311 of all patients (30.7%) underwent surgical procedures while the other 703 patients (69.3%) required no surgery (Table 1).
Trauma is the most common cause ofdisabilities among the young populationin developing countries [1]. Aside from morbidity and mortality, traumaticinjuries can significantly decrease thequality of life and life expectancy of the victims. Traumatic injuries are mostcommon in the younger working population but they arealso high among the older population [2]. Spinal column injuries are rare, but they can cause high mortality andmorbidity rates with heavy burdens and lifelong social, financial, and personal problems and even permanent disabilities [3]. Traumatic spinal column injuries are alsohigh in low socio-economic areas due to frequent use of motorcycles, lack of sufficient immunity, and absence of adequate infrastructures.
Traumatic Spinal Cord Injury (TSCI) can occur afterspinal column injury [4]. TSCI is an acute, traumatic lesion of the spinal cord with its consequent economic problems and can emotionally and psychologically affect the patients. It can affect different systems andorgans of the body and cause motor or sensory impairmentsor dysfunction of urinary, gastrointestinal, or reproductivesystems [5]. TSCI in pediatric or young populationis a catastrophic event that can alter the child’s life forever. Different studies had surveys about the incidence of TSCI around the world and this incidence ranges from 3.6 to 195.4 patients per million around the world [6].
Studies indicate that TSCI is mostly caused by vehicle accidents, falling, and violence. Age distribution for TSCI also showed a higher incidence in 15-29 and over65 years old people [7]. These data indicate the importance of TSCI because it affects mostly younger working population causing heavy socio-economic burden and older population in whom serious complications are observed. TSCI can permanently damage different organs but they may be rehabilitated by the means of physiotherapies or occupational therapies [8]. Evidence shows that early surgical intervention in cases that require immediate surgery could be a great help in further prognosis [9]. Different studies surveyed the epidemiology of TSCI and evaluated age and sex distributions and relatedfactors. This study aims to evaluate spinal column fractures based on anatomical position, percentage of TSCI, and need for surgery in Iran. This information can enrich our knowledge of spinal cord trauma and safety considerations at the scene of the accident.
2. Methods
This is a retrospective study of cases with traumatic spinal column fractures referring to Al-Zahra Hospital, one of the most important trauma centers of Isfahan City, Iran. We evaluated all cases diagnosed with traumaticspinal column fractures between 2012 and 2018. A total of 1014 patients were included in our study. The exclusion criteria were lacking clear spine radiology images or patients with severe brain injury. The study was approved by the Ethics Committee of Isfahan University of Medical Sciences. All medical records of patients were reviewed and anatomical locations of spine fractureswere evaluated. Patients with spinal cord injuries were also detected based on documented history andMRI findings. The need for surgery and the percentage of TSCI were also evaluated. The obtained data wereanalyzed in SPSS.
3. Results
In this study, 1014 patients with traumatic spinal columnfractures were included. The most common causes of trauma were vehicle and road accidents (83.4%) followed by falling (12.7%). Sex distribution indicated that 717 cases (70.7%) were male and 297 (29.3%) female. Furthermore, 7.1% of male patients had spinal injurieswhile only 3.7% of females had spinal injuries and thisdifference was statistically significant (P=0.024). A total of 21 patients (2.1%) died due to injuries. Statistics showed that 85.7% of mortalities occurred in males and 14.3% in females and as a result, male patients with traumatic spine injuries had higher mortalities. The frequencyof TSCI among patients with traumatic spinal column fractures were 62 patients (6.1%). Further analysis also indicated that 311 of all patients (30.7%) underwent surgical procedures while the other 703 patients (69.3%) required no surgery (Table 1).
The frequency of eachtype of fracture was also evaluated. The single-level fracture was found in 92.3% of patients, comprising cervical spine fractures in 16.0% (74.1% in males and 25.9% in females), thoracic spine fractures in 27.4% (76.3% in males and 23.7% in females), lumbar spine fractures in 38.3% (67.8% in males and 32.2% in females), sacrum and coccyx fractures in 10.7% (59.3% in males and 40.7% in females). The multiple fractures were seen in7.7% of patients (74.4% in males and 25.6% in females). These results indicate that lumbar spine fractures especially in men are the most common fractures in traumatic spinal fractures.
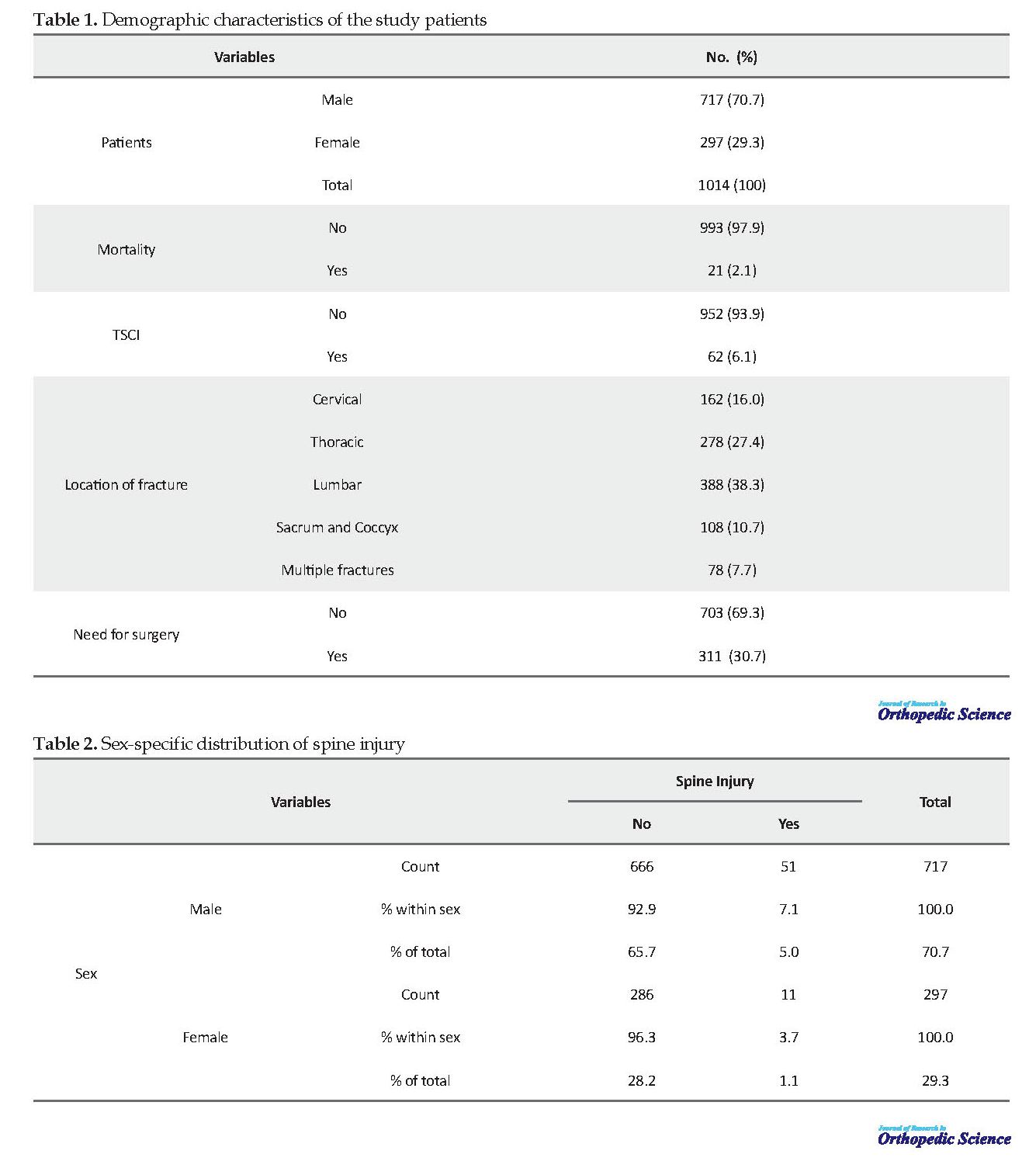
Sex distribution for TSCI indicated that 7.1% of all male patients with spinal column fractures had TSCI while for female patients this rate was 3.7% (Table 2). Our data also indicated that 67.7% of patients with TSCI underwent surgery. Analysis for distribution of spinal injuries among different sites of spinal column fractures indicated that cervical spines had the highest incidence of TSCI (43.5% of all TSCIs) followed by thoracic spines fractures (29% of all TSCIs). For lumbar spines fractures, 24.2% of patients faced TSCI andsacral fractures associated with no TSCI. The percentage of TSCI among patients with multiple site fractures was 3.2% (Table 3).
Sex distribution for TSCI indicated that 7.1% of all male patients with spinal column fractures had TSCI while for female patients this rate was 3.7% (Table 2). Our data also indicated that 67.7% of patients with TSCI underwent surgery. Analysis for distribution of spinal injuries among different sites of spinal column fractures indicated that cervical spines had the highest incidence of TSCI (43.5% of all TSCIs) followed by thoracic spines fractures (29% of all TSCIs). For lumbar spines fractures, 24.2% of patients faced TSCI andsacral fractures associated with no TSCI. The percentage of TSCI among patients with multiple site fractures was 3.2% (Table 3).
Furthermore, we found that thoracicand cervical spine fractures were mostly associated with high mortality compared with other sites of spine fractures (47.6% and 38.1% of all mortalities, respectively). It should also be noted that lumbar spine fractures were associated with no mortality among all fractures (Table 4). Age analysis for fractures of the spinal column indicated that the Mean±SD age for cervical spine fractures is 39.86±17.43 years. For thoracic spine fractures, this figure is 39.68±18.54 years. The Mean±SD age for lumbar spine fractures is 40.02±16.61 years. For sacrum and coccyx fractures, it is 36.91±17.42 years and for multiple fractures 38.60±17.42 years. Thus, patients with sacrum and coccyx fractures have the lowest mean age and those with lumbar fractures have the highest mean age.
4. Discussion
The results of our study indicated a prevalence of 6.1% for TSCI among patients with spinal column fractures. The mortality rate of our patients was 2.1% and the most common fractures were lumbar and thoracic spine fractures. About 67.7% of our patients with TSCI required surgical treatments. Furthermore, we found that lumbar spine fractures had the highest incidence of TSCI while thoracic and cervical spine fractures were associatedwith the highest mortality rate. Our analysis also indicated that mortality rates are higher among male patients with cervical fractures with the Mean±SD age of 39.86±17.43 years.
Falavigna et al. had recently surveyed the epidemiology of fractures and TSCI among patients younger than18 years [10]. Their results indicated that TSCI occurred in 52.6% of patients. Most injured sites of the spinal column were lower thoracic levels and they also indicated that 73.9% of patients underwent surgical procedures. However, the percentage of TSCI in our study was 6.1% and the most common injured site was lumbar vertebrae.We also showed that 30.7% of our cases needed surgical treatments. These differences in data are possibly due to age and other epidemiological differences. The most common causes of spinal injuries in the Falavigna's study was falling while our patients were mostly injured by vehicle and road accidents.
Hagen reported that higher thoracic spine injuries are associated with grater complications [11]. This findingis in line with our data showing a higher mortality ratein patients with thoracic and cervical spine injuries. Majdan et al. also conducted an epidemiological study on patients with TSCI [7]. They reported that cervical trauma was the most common injured region (52%). They also reported that TSCI has a higher incidence in patients older than 65 years who face spinal injuries. In most studies,which were performed in developed countries, the main cause of the spinal column accident is falling [12, 13] but in our study, most cases (83.4%) were injured by road accidents which indicate the poor vehicle and road safety in Iran. The differences between our data and other studies could be mostly due to this factor.
In this study, the mortality rate of patients was 2.1% of all cases and we found that thoracic and cervical spinefractures were mostly associated with high mortalitycompared with other sites of spine fractures. Löfvenmark et al. also surveyed the epidemiologic features of TSCI and reported a 20% mortality rate [14]. They also reported that the most common cause of TSCI was roadtraffic accidents. These data are in line with our study but we reported a lower rate of mortality which might be due to lower intensity of trauma and TSCI. Investigating a long-term follow-up of patients with TSCI, Savic et al. published a report indicating an improved life expectancy of patients with TSCI [5]. They also had a survey on risk factors for mortality among these patients.Gender, current age, time since injury, and neurological grouping were the most important risks for long term mortality among patients with TSCI. The limitations ofthis study were lack of sufficient personal resources andincomplete documents of some patients, so our research team had to check some cases in person.
5. Conclusion
Taken together, we found that the epidemiological features of spinal column injuries and TSCI vary among different societies due to different causes. So far, this study is the first study to evaluate different spine fractures and TSCI and other associated factors in the Iranian population. Our results indicate a high incidence of thoracic and lumbar spine fractures and higher mortality rates in thoracic and cervical spine fractures.
Ethical Considerations
Compliance with ethical guidelines
The review board approved this research of our institute under the (Code: 397094). The written consent was obtained from the patients before their participation in the study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization: Hossein Akbari Aghdam, Ali Andalib; Methodology, investigation: All authors; Writing-Original Draft Preparation: Emran Ahmadi, Hossein Akbari Aghdam; Writing review and editing : All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Kafer A. Un/safe disclosures: Scenes of disability and trauma. J Lit & Cult Disabil Stud. 2016; 10(1):1-20. [DOI:10.3828/jlcds.2016.1]
Palmer CS, Gabbe BJ, Cameron PA. Defining major trauma using the 2008 Abbreviated Injury Scale. Inj. 2016; 47(1):109-15. [DOI:10.1016/j.injury.2015.07.003] [PMID]
Niemi-Nikkola V, Saijets N, Ylipoussu H, Kinnunen P, Pesälä J, Mäkelä P, et al. Traumatic spinal injuries in Northern Finland. Spine. 2018; 43(1):E45-E51. [DOI:10.1097/BRS.0000000000002214] [PMID]
Ahuja CS, Wilson JR, Nori S, Kotter MR, Druschel C, Curt A, et al. Traumatic spinal cord injury. Nat Rev Dis Primers. 2017; 3:17018. [DOI:10.1038/nrdp.2017.18] [PMID]
Savic G, DeVivo M, Frankel H, Jamous M, Soni B, Charlifue S. Long-term survival after traumatic spinal cord injury: A 70-year British study. Spinal Cord. 2017; 55(7):651. [DOI:10.1038/sc.2017.23] [PMID]
Jazayeri SB, Beygi S, Shokraneh F, Hagen EM, Rahimi-Movaghar V. Incidence of traumatic spinal cord injury worldwide: A systematic review. Eur Spine J. 2015; 24(5):905-18. [DOI:10.1007/s00586-014-3424-6] [PMID]
Majdan M, Brazinova A, Mauritz W. Epidemiology of traumatic spinal cord injuries in Austria 2002-2012. Eur Spine J. 2016; 25(1):62-73. [DOI:10.1007/s00586-015-3985-z] [PMID]
Nas K, Yazmalar L, Şah V, Aydın A, Öneş K. Rehabilitation of spinal cord injuries. World J Orthop. 2015; 6(1):8. [DOI:10.5312/wjo.v6.i1.8]
Grassner L, Wutte C, Klein B, Mach O, Riesner S, Panzer S, et al. Early decompression (< 8 h) after traumatic cervical spinal cord injury improves functional outcome as assessed by spinal cord independence measure after one year. J Neurotrauma. 2016; 33(18):1658-66. [DOI:10.1089/neu.2015.4325] [PMID]
Falavigna A, Righesso O, da Silva PG, Chavez FAS, Sfreddo E, de Almeida LP, et al. Epidemiology and management of spinal trauma in children and adolescents< 18 years old. World Neurosurg. 2018; 110:e479-e83. [DOI:10.1016/j.wneu.2017.11.021] [PMID]
Hagen EM. Acute complications of spinal cord injuries. World J Orthop. 2015; 6(1):17. [DOI:10.5312/wjo.v6.i1.17] [PMID] [PMCID]
Joseph C, Andersson N, Bjelak S, Giesecke K, Hultling C. Incidence, aetiology and injury characteristics of traumatic spinal cord injury in Stockholm, Sweden: A prospective, population-based update. J Rehabil Med. 2017; 49(5):431-6. [DOI:10.2340/16501977-2224] [PMID]
Chamberlain JD, Deriaz O, Hund-Georgiadis M, Meier S, Scheel-Sailer A, Schubert M, et al. Epidemiology and contemporary risk profile of traumatic spinal cord injury in Switzerland. Inj Epidemiol. 2015; 2(1):28. [DOI:10.1186/s40621-015-0061-4] [PMID] [PMCID]
Löfvenmark I, Norrbrink C, Nilsson-Wikmar L, Hultling C, Chakandinakira S, Hasselberg M. Traumatic spinal cord injury in Botswana: Characteristics, aetiology and mortality. Spinal Cord. 2015; 53(2):150. [DOI:10.1038/sc.2014.203] [PMID]
4. Discussion
The results of our study indicated a prevalence of 6.1% for TSCI among patients with spinal column fractures. The mortality rate of our patients was 2.1% and the most common fractures were lumbar and thoracic spine fractures. About 67.7% of our patients with TSCI required surgical treatments. Furthermore, we found that lumbar spine fractures had the highest incidence of TSCI while thoracic and cervical spine fractures were associatedwith the highest mortality rate. Our analysis also indicated that mortality rates are higher among male patients with cervical fractures with the Mean±SD age of 39.86±17.43 years.
Falavigna et al. had recently surveyed the epidemiology of fractures and TSCI among patients younger than18 years [10]. Their results indicated that TSCI occurred in 52.6% of patients. Most injured sites of the spinal column were lower thoracic levels and they also indicated that 73.9% of patients underwent surgical procedures. However, the percentage of TSCI in our study was 6.1% and the most common injured site was lumbar vertebrae.We also showed that 30.7% of our cases needed surgical treatments. These differences in data are possibly due to age and other epidemiological differences. The most common causes of spinal injuries in the Falavigna's study was falling while our patients were mostly injured by vehicle and road accidents.
Hagen reported that higher thoracic spine injuries are associated with grater complications [11]. This findingis in line with our data showing a higher mortality ratein patients with thoracic and cervical spine injuries. Majdan et al. also conducted an epidemiological study on patients with TSCI [7]. They reported that cervical trauma was the most common injured region (52%). They also reported that TSCI has a higher incidence in patients older than 65 years who face spinal injuries. In most studies,which were performed in developed countries, the main cause of the spinal column accident is falling [12, 13] but in our study, most cases (83.4%) were injured by road accidents which indicate the poor vehicle and road safety in Iran. The differences between our data and other studies could be mostly due to this factor.
In this study, the mortality rate of patients was 2.1% of all cases and we found that thoracic and cervical spinefractures were mostly associated with high mortalitycompared with other sites of spine fractures. Löfvenmark et al. also surveyed the epidemiologic features of TSCI and reported a 20% mortality rate [14]. They also reported that the most common cause of TSCI was roadtraffic accidents. These data are in line with our study but we reported a lower rate of mortality which might be due to lower intensity of trauma and TSCI. Investigating a long-term follow-up of patients with TSCI, Savic et al. published a report indicating an improved life expectancy of patients with TSCI [5]. They also had a survey on risk factors for mortality among these patients.Gender, current age, time since injury, and neurological grouping were the most important risks for long term mortality among patients with TSCI. The limitations ofthis study were lack of sufficient personal resources andincomplete documents of some patients, so our research team had to check some cases in person.
5. Conclusion
Taken together, we found that the epidemiological features of spinal column injuries and TSCI vary among different societies due to different causes. So far, this study is the first study to evaluate different spine fractures and TSCI and other associated factors in the Iranian population. Our results indicate a high incidence of thoracic and lumbar spine fractures and higher mortality rates in thoracic and cervical spine fractures.
Ethical Considerations
Compliance with ethical guidelines
The review board approved this research of our institute under the (Code: 397094). The written consent was obtained from the patients before their participation in the study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization: Hossein Akbari Aghdam, Ali Andalib; Methodology, investigation: All authors; Writing-Original Draft Preparation: Emran Ahmadi, Hossein Akbari Aghdam; Writing review and editing : All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Kafer A. Un/safe disclosures: Scenes of disability and trauma. J Lit & Cult Disabil Stud. 2016; 10(1):1-20. [DOI:10.3828/jlcds.2016.1]
Palmer CS, Gabbe BJ, Cameron PA. Defining major trauma using the 2008 Abbreviated Injury Scale. Inj. 2016; 47(1):109-15. [DOI:10.1016/j.injury.2015.07.003] [PMID]
Niemi-Nikkola V, Saijets N, Ylipoussu H, Kinnunen P, Pesälä J, Mäkelä P, et al. Traumatic spinal injuries in Northern Finland. Spine. 2018; 43(1):E45-E51. [DOI:10.1097/BRS.0000000000002214] [PMID]
Ahuja CS, Wilson JR, Nori S, Kotter MR, Druschel C, Curt A, et al. Traumatic spinal cord injury. Nat Rev Dis Primers. 2017; 3:17018. [DOI:10.1038/nrdp.2017.18] [PMID]
Savic G, DeVivo M, Frankel H, Jamous M, Soni B, Charlifue S. Long-term survival after traumatic spinal cord injury: A 70-year British study. Spinal Cord. 2017; 55(7):651. [DOI:10.1038/sc.2017.23] [PMID]
Jazayeri SB, Beygi S, Shokraneh F, Hagen EM, Rahimi-Movaghar V. Incidence of traumatic spinal cord injury worldwide: A systematic review. Eur Spine J. 2015; 24(5):905-18. [DOI:10.1007/s00586-014-3424-6] [PMID]
Majdan M, Brazinova A, Mauritz W. Epidemiology of traumatic spinal cord injuries in Austria 2002-2012. Eur Spine J. 2016; 25(1):62-73. [DOI:10.1007/s00586-015-3985-z] [PMID]
Nas K, Yazmalar L, Şah V, Aydın A, Öneş K. Rehabilitation of spinal cord injuries. World J Orthop. 2015; 6(1):8. [DOI:10.5312/wjo.v6.i1.8]
Grassner L, Wutte C, Klein B, Mach O, Riesner S, Panzer S, et al. Early decompression (< 8 h) after traumatic cervical spinal cord injury improves functional outcome as assessed by spinal cord independence measure after one year. J Neurotrauma. 2016; 33(18):1658-66. [DOI:10.1089/neu.2015.4325] [PMID]
Falavigna A, Righesso O, da Silva PG, Chavez FAS, Sfreddo E, de Almeida LP, et al. Epidemiology and management of spinal trauma in children and adolescents< 18 years old. World Neurosurg. 2018; 110:e479-e83. [DOI:10.1016/j.wneu.2017.11.021] [PMID]
Hagen EM. Acute complications of spinal cord injuries. World J Orthop. 2015; 6(1):17. [DOI:10.5312/wjo.v6.i1.17] [PMID] [PMCID]
Joseph C, Andersson N, Bjelak S, Giesecke K, Hultling C. Incidence, aetiology and injury characteristics of traumatic spinal cord injury in Stockholm, Sweden: A prospective, population-based update. J Rehabil Med. 2017; 49(5):431-6. [DOI:10.2340/16501977-2224] [PMID]
Chamberlain JD, Deriaz O, Hund-Georgiadis M, Meier S, Scheel-Sailer A, Schubert M, et al. Epidemiology and contemporary risk profile of traumatic spinal cord injury in Switzerland. Inj Epidemiol. 2015; 2(1):28. [DOI:10.1186/s40621-015-0061-4] [PMID] [PMCID]
Löfvenmark I, Norrbrink C, Nilsson-Wikmar L, Hultling C, Chakandinakira S, Hasselberg M. Traumatic spinal cord injury in Botswana: Characteristics, aetiology and mortality. Spinal Cord. 2015; 53(2):150. [DOI:10.1038/sc.2014.203] [PMID]
Type of Study: Research Article |
Subject:
Hand surgery / Elbow
Received: 2020/03/1 | Accepted: 2020/05/12 | Published: 2020/05/30
Received: 2020/03/1 | Accepted: 2020/05/12 | Published: 2020/05/30
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
