



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jros.iums.ac.ir/article-1-2113-en.html



1. Introduction
Carpal bone fractures are probably more common than reported. It accounts for a significant proportion of injuries to the wrist. Its complex bone shape and articulations make the diagnosis of fractures more difficult and missed injuries are common.
Among the fractures of the wrist, physicians mostly pay attention to the scaphoid bone with respect to the frequency of involvement as well as prognosis [1].
Isolated fractures of the trapezoid bone have been rarely reported in the literature. The mechanism of injury is an axial or bending load transmitted through the second metacarpal [2, 3].
This study aimed to present a rare case of a trapezoid fracture associated with a scaphoid fracture.
2. Case Presentation
A 31-year-old male presented to the emergency department with right wrist pain following a high-velocity motor vehicle accident. On physical examination of the affected right upper extremity, the patient had wrist swelling.
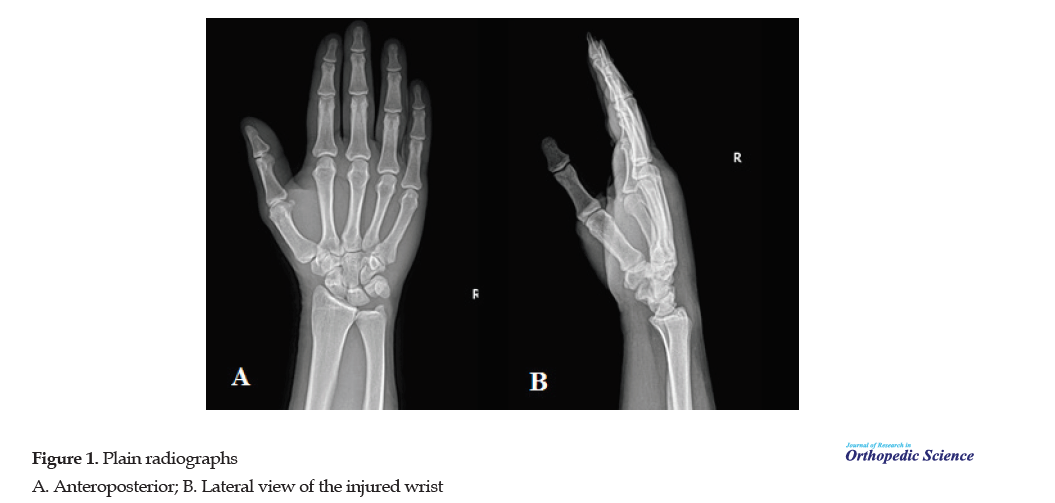
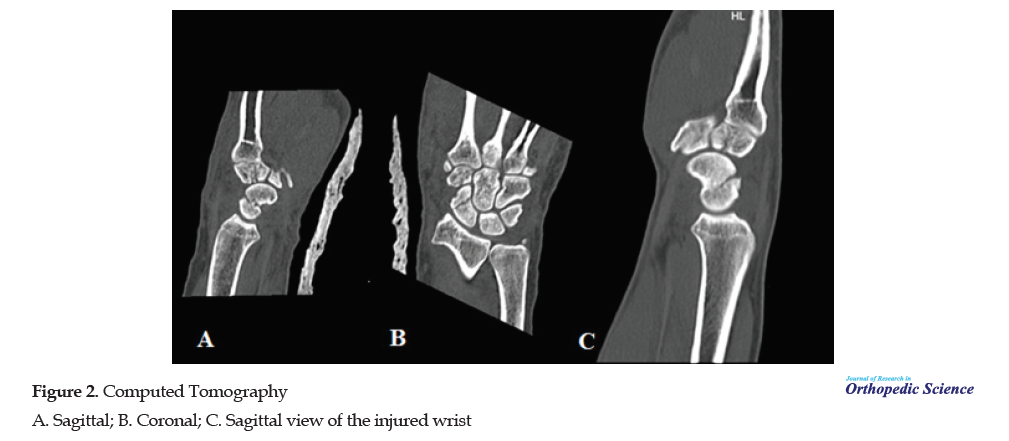
There was tenderness to palpation at the base of the second metacarpal and snuff box. Because of pain, the patient had limited wrist flexion, wrist extension, and radial-ulnar deviation. The patient’s right wrist and hand were neurovascularly intact. Wrist x-rays (Figure 1) and computed tomography (Figure 2) demonstrated a nondisplaced proximal trapezoid bone fracture and concomitant obliquely oriented nondisplaced fracture of the scaphoid.
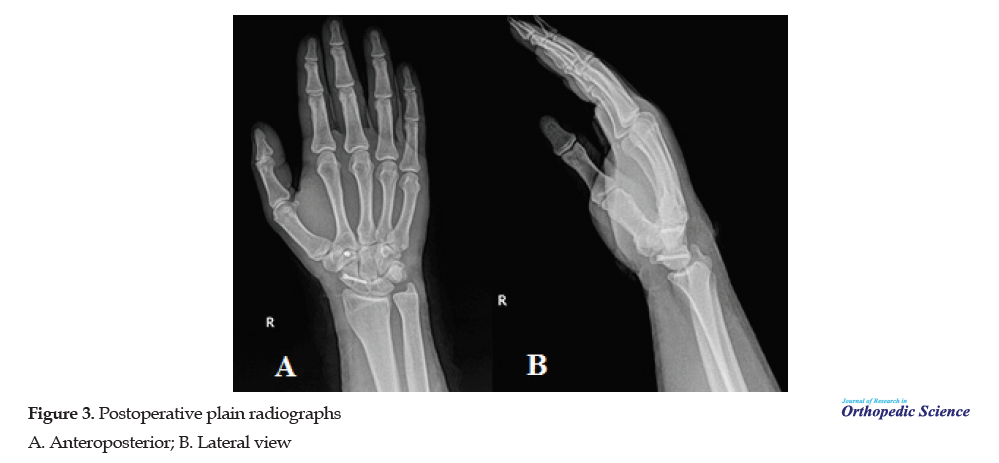
Surgery was performed 3 days after the patient’s initial hospital visit. The hand was placed on a radiolucent table with the shoulder abducted and the forearm in supination. The wrist was extended over a roll. A 4- to 5-mm skin incision was made about 1 cm distal and radial to the scaphoid tubercle and the tip of the guidewire was placed on the scaphoid tubercle. The guidewire was inserted at a 45-degree angle, visualizing the anteroposterior plane with a fluoroscope. A second wire was inserted to support the fracture site and avoid rotational deformity. The length of the screw was then measured and a 20-mm screw, which was self-drilling and self-tapping, was inserted. Another 4- to 5-mm skin incision was made over the trapezoid and the guidewire was inserted perpendicularly and a 10-mm screw was inserted under fluoroscopic control (Figure 3, 4).
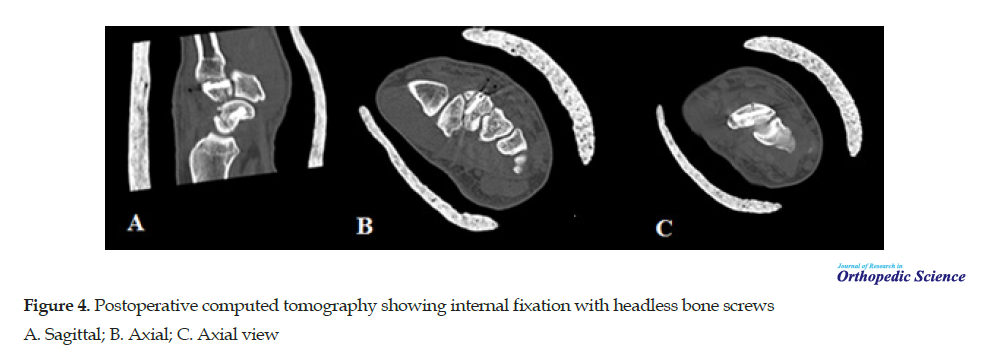
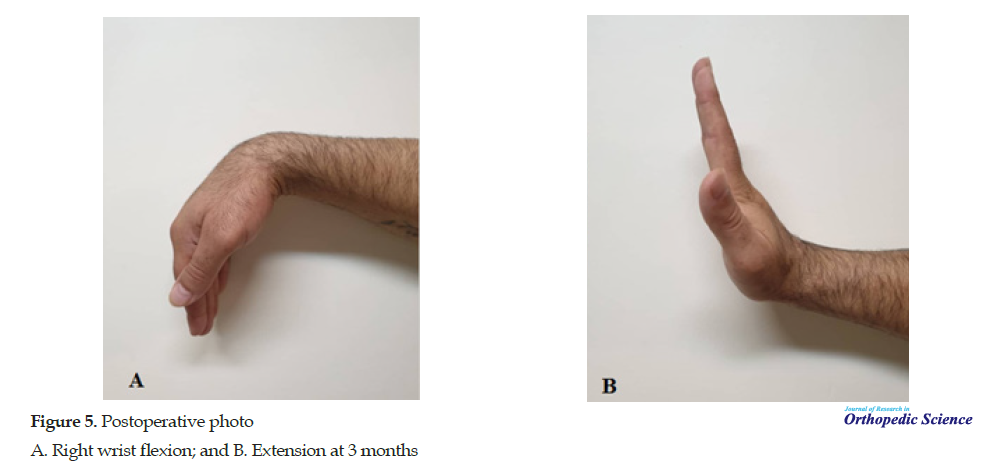
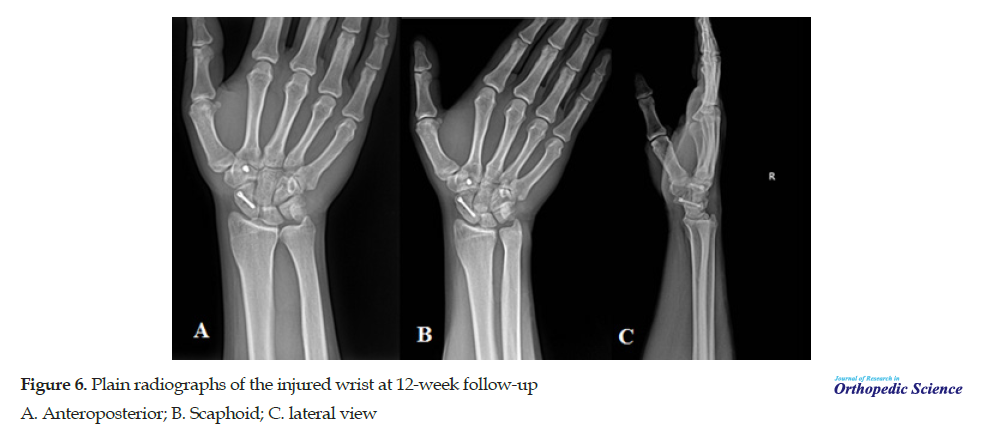
Postoperatively, a sugar-tong splint was applied. He also began hand physiotherapy, which included a passive and active range of motion 4 weeks after surgery. At 12-month follow-up, the patient reported a full return to baseline function (Figure 5, 6).
3. Discussion
Trapezoidal fractures are the rarest carpal fractures, at less than 1% rate. To date, only one article has been published in English on trapezoid fracture associated with scaphoid fracture. In May 2019, Yamamoto et al. presented the first trapezoid fracture associated with a scaphoid fracture in a football goalkeeper [4]. So far, the proposed mechanisms of isolated trapezoid fracture essentially center on high-energy axial or bending mechanism transmitted through the index metacarpal proximally [5-8]. The axial load of index metacarpal could be transmitted to the scaphoid via the trapezoid, leading to the fractures of both of them.
Gruson KI reported isolated trapezoid fractures. They believed the mechanism of injury was an axial or bending load transmitted through the second metacarpal.
The patient had a nondisplaced trapezoid fracture that was sustained by direct trauma and subsequently treated successfully in a short-arm cast [9].
In the examination of trauma, it is important to suspect a carpal bone fracture. Thus examining physicians must enter the trapezoid fracture in their differential of posttraumatic, radial-sided wrist pain, and be willing to investigate further through the judicious use of imaging studies.
We feel that this combination of fracture will continue to remain an uncommon entity and a high index of suspicion must be aroused on the part of the examiner based on the reported mechanism and physical findings.
4. Conclusion
We presented a rare case of a trapezoid fracture associated with a scaphoid fracture. The axial load of index metacarpal could be transmitted to the scaphoid via the trapezoid, leading to the fractures of both of them.
Ethical Considerations
Compliance with ethical guidelines
Written consent was obtained from the patient for publication of this case report. A copy of the written consent is available for review.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
References
1.Sadowski RM, Montilla RD. Rare isolated trapezoid fracture: A case report. Hand. 2008; 3(4):372-4. [DOI:10.1007/s11552-008-9100-8] [PMID] [PMCID]
2.Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH. Green’s Operative Hand Surgery. Amsterdam: Elsevier Health Sciences; 2010.
3.Garcia-Elias M. Carpal bone fractures (excluding scaphoid fractures). Philadelphia: Lippincott Williams & Wilkins; 2001.
4.Yamamoto T, Matsushita T, Ito K, Matsushima S, Yoshida K, Kuroda R. Trapezoid fracture associated with scaphoid fracture in a football goalkeeper. Case Rep Orthop. 2019; 2019:7949754. [DOI:10.1155/2019/7949754] [PMID] [PMCID]
5.Jeong G, Kram D, Lester B. Isolated fracture of the trapezoid. Am J Orthop. 2001; 30(3):228-30.
6.Nijs S, Mulier T, Broos P. Occult fracture of the trapezoid bone: A report on two cases. Acta Orthop Belg. 2004; 70(2):177-9.
7.Miyawaki T, Kobayashi M, Matsuura S, Yanagawa H, Imai T, Kurihara K. Trapezoid bone fracture. Annals of plastic surgery. 2000; 44(4):444-6. [DOI:10.1097/00000637-200044040-00017] [PMID]
8.Watanabe H, Hamada Y, Yamamoto Y. A case of old trapezoid fracture. Arch Orthop Trauma Surg. 1999; 119(5-6):356-7. [DOI:10.1007/s004020050427] [PMID]
9.Gruson KI, Kaplan KM, Paksima N. Isolated trapezoid fractures: A case report with compilation of the literature. Bull NYU Hosp Jt Dis. 2008; 66:(1):57-60.
Received: 2020/05/21 | Accepted: 2020/07/23 | Published: 2020/08/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
