

Volume 9, Issue 2 (5-2022)
JROS 2022, 9(2): 119-122 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shariatzadeh H, Mirzaei A, Hosseinzade D. Ganglion Cyst of the Thenar Muscle: A Case Report. JROS 2022; 9 (2) :119-122
URL: http://jros.iums.ac.ir/article-1-2203-en.html
URL: http://jros.iums.ac.ir/article-1-2203-en.html



1- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 1039 kb]
(261 Downloads)
| Abstract (HTML) (1390 Views)
Full-Text: (398 Views)
1. Introduction
Ganglion cysts are lesions that grow in the joint capsule or tendon sheaths. These lesions are the most common type of soft tissue tumors in the hands, wrists, and feet (50% to 70%). It is more common in women (70%) [1, 2, 3, 4]. Medical concerns include the cosmetic appearance of the mass, pain, weakness, and malignancy. This lesion subsides with rest and enlarges with activity and, in most cases, disappears spontaneously. Surgical excision has a lower risk of recurrence compared to aspiration [5].
Ganglion cysts are mainly located in areas that are easily detected by hand surgeons. The differential diagnosis for swelling of the dorsal side of the wrist is extensor tenosynovitis, lipomas, and other hand tumors [6]. Rarely ganglion cyst is presented in unusual locations, such as the lunate, scaphoid, and intra-tendinous portion [3, 7]. Involvement of the thenar muscle is very rare and has been reported in only two previous studies.
Here, we report a ganglion cyst of the thenar muscle in a 25-year-old woman, which was located adjacent to the recurrent branch of the median nerve.
2. Case Presentation
A 25-year-old woman presented to our orthopedic clinic with a progressively growing mass over the palmar aspect of her left and non-dominant hand from one year ago without increasing pain. She had no history of specific trauma. On physical examination, the patient had a firm, mobile, non-tender mass on the volar aspect of the radial side of the hand, in the periphery of the thenar muscles. The thenar muscle power was good (grade 5). She had no sensory deficits in the palmar surfaces of her thenar muscle and digits. The approximate size of the lesion in palpation was 1×1 cm. No limitation exists in the range of motion of the wrist.
Radiographic evaluation with plain X-rays did not show fracture or acute abnormalities. Magnetic resonance imaging (MRI) without gadolinium contrast revealed a cystic mass on the volar aspect of the hand, adjacent to the thenar muscles. The lesion was well-circumscribed, with a size of 2×2×1 cm and low signal intensity on T2 sequences (Figure 1).
 The patient was taken to the operating room, and the median nerve was explored with an incision at the volar side of the wrist parallel to the thenar crease. A cystic mass was found at the depth of the digital nerve and the recurrent branch of the median nerve in the muscle fiber of the thenar muscle (Figure 2).
The patient was taken to the operating room, and the median nerve was explored with an incision at the volar side of the wrist parallel to the thenar crease. A cystic mass was found at the depth of the digital nerve and the recurrent branch of the median nerve in the muscle fiber of the thenar muscle (Figure 2).
 By protecting the recurrent branch of the median and digital nerve, the mass was excised and sent to the pathology department. Macroscopic evaluation of the mass revealed a 2.5×1×0.5 cm lesion with a smooth inner surface and without papillary projections (Figure 3a).
By protecting the recurrent branch of the median and digital nerve, the mass was excised and sent to the pathology department. Macroscopic evaluation of the mass revealed a 2.5×1×0.5 cm lesion with a smooth inner surface and without papillary projections (Figure 3a).
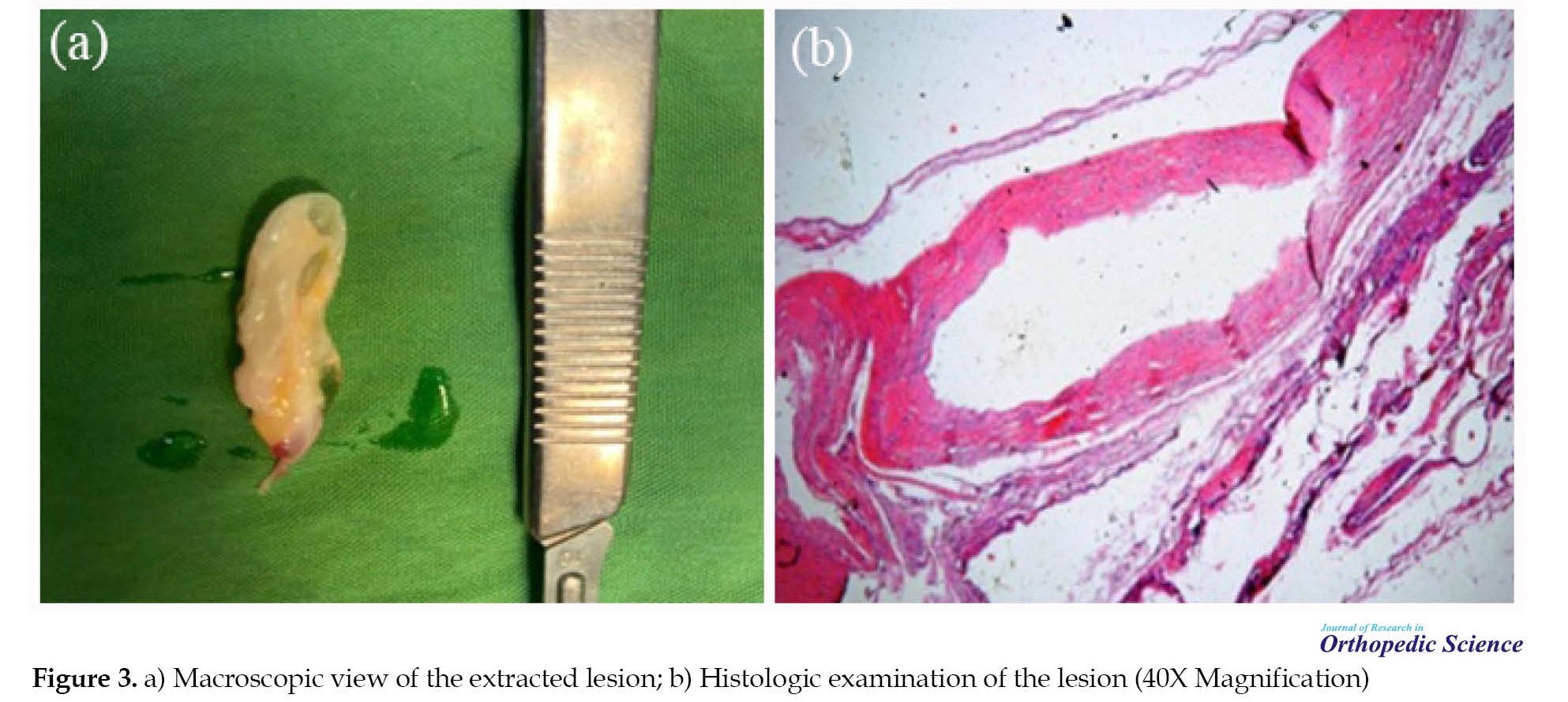 Histologic evaluation showed a multilocular cystic structure composed of dense collagenous walls without true epithelial lining with foci of myxoid change (Figure 3b). Accordingly, the diagnosis of a ganglion cyst was made.
Histologic evaluation showed a multilocular cystic structure composed of dense collagenous walls without true epithelial lining with foci of myxoid change (Figure 3b). Accordingly, the diagnosis of a ganglion cyst was made.
The patient remained symptom-free during the six months postoperatively. The clinical and radiological recurrence was not observed during the follow-up period. The patient provided written informed consent to use her medical data for publication.
3. Discussion
Treatment of benign lesions can be difficult, particularly if presented in rare locations [8, 9]. The dorsal wrist is the most common location of the hand and wrist ganglia (up to 70%). Other common locations are the volar-radial wrist, the dorsal side of the distal interphalangeal joint (mucous cyst), and the volar proximal digital flexion crease (flexor retinacular cyst). Approximately 90% of volar wrist ganglia arise from the radioscaphoid or scaphotrapezial joint [10]. The thenar of the hand is a rare location for a ganglion cyst. The literature review retrieved two articles describing a volar wrist ganglion at the thenar muscle. In 1993, Chiu and Aschermann reported the first case of a ganglion in the thenar muscle [11]. Azzopardi et al. reported the second case of ganglion cyst originated from the first carpometacarpal joint and rapidly expanded to the thenar eminence ganglion. At first glance, it mimicked a sarcoma [12].
Here, we presented a ganglion cyst originating from the tendon of the thenar muscle. It is essential to differentiate ganglion cysts of unusual locations from other diagnoses to avoid overtreatment of the patients. MRI can be very useful for this purpose. On the T2-weighted MRI, ganglion cysts can be characterized by a lobular, multiseptated, and hyperintense signal covering the whole lesion. Ultrasound evaluation can also be useful in the differentiation of ganglion cysts from other soft tissue lesions [13, 14]. In the present report, we only used MRI for diagnosis.
Treatment of ganglion cysts includes a conservative approach or surgical intervention. In symptomatic cases, surgical excision is the treatment of choice. Also, in cases with atypical localization, difficult needle aspiration, and a high risk of recurrence, surgical resection is recommended. Post-excision recurrence may occur due to the inadequate resection of the tumor mass.
Although atypical localization of ganglion cysts rarely occurs, it should be considered in the differential diagnosis of hand and wrist lesions. In our case, the growth speed and clinical course did not raise the clinical suspicion of malignancy. However, due to the proximity of the mass in the thenar area and its proximity to the crucial adjacent structures, including the recurrent branch of the median nerve and digital nerve, early and accurate diagnosis and treatment through timely clinical investigation and complete preoperative imaging analysis are required.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research and considering that the article is a case report and that the university has not defined a code of ethics for this type of article, the research has been done with the patient's consent at all stages.
Funding
The article is the result of the author's research at the Bone and Joint Research Center of Shafaihiyaian Hospital, Iran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Ganglion cysts are lesions that grow in the joint capsule or tendon sheaths. These lesions are the most common type of soft tissue tumors in the hands, wrists, and feet (50% to 70%). It is more common in women (70%) [1, 2, 3, 4]. Medical concerns include the cosmetic appearance of the mass, pain, weakness, and malignancy. This lesion subsides with rest and enlarges with activity and, in most cases, disappears spontaneously. Surgical excision has a lower risk of recurrence compared to aspiration [5].
Ganglion cysts are mainly located in areas that are easily detected by hand surgeons. The differential diagnosis for swelling of the dorsal side of the wrist is extensor tenosynovitis, lipomas, and other hand tumors [6]. Rarely ganglion cyst is presented in unusual locations, such as the lunate, scaphoid, and intra-tendinous portion [3, 7]. Involvement of the thenar muscle is very rare and has been reported in only two previous studies.
Here, we report a ganglion cyst of the thenar muscle in a 25-year-old woman, which was located adjacent to the recurrent branch of the median nerve.
2. Case Presentation
A 25-year-old woman presented to our orthopedic clinic with a progressively growing mass over the palmar aspect of her left and non-dominant hand from one year ago without increasing pain. She had no history of specific trauma. On physical examination, the patient had a firm, mobile, non-tender mass on the volar aspect of the radial side of the hand, in the periphery of the thenar muscles. The thenar muscle power was good (grade 5). She had no sensory deficits in the palmar surfaces of her thenar muscle and digits. The approximate size of the lesion in palpation was 1×1 cm. No limitation exists in the range of motion of the wrist.
Radiographic evaluation with plain X-rays did not show fracture or acute abnormalities. Magnetic resonance imaging (MRI) without gadolinium contrast revealed a cystic mass on the volar aspect of the hand, adjacent to the thenar muscles. The lesion was well-circumscribed, with a size of 2×2×1 cm and low signal intensity on T2 sequences (Figure 1).
The patient remained symptom-free during the six months postoperatively. The clinical and radiological recurrence was not observed during the follow-up period. The patient provided written informed consent to use her medical data for publication.
3. Discussion
Treatment of benign lesions can be difficult, particularly if presented in rare locations [8, 9]. The dorsal wrist is the most common location of the hand and wrist ganglia (up to 70%). Other common locations are the volar-radial wrist, the dorsal side of the distal interphalangeal joint (mucous cyst), and the volar proximal digital flexion crease (flexor retinacular cyst). Approximately 90% of volar wrist ganglia arise from the radioscaphoid or scaphotrapezial joint [10]. The thenar of the hand is a rare location for a ganglion cyst. The literature review retrieved two articles describing a volar wrist ganglion at the thenar muscle. In 1993, Chiu and Aschermann reported the first case of a ganglion in the thenar muscle [11]. Azzopardi et al. reported the second case of ganglion cyst originated from the first carpometacarpal joint and rapidly expanded to the thenar eminence ganglion. At first glance, it mimicked a sarcoma [12].
Here, we presented a ganglion cyst originating from the tendon of the thenar muscle. It is essential to differentiate ganglion cysts of unusual locations from other diagnoses to avoid overtreatment of the patients. MRI can be very useful for this purpose. On the T2-weighted MRI, ganglion cysts can be characterized by a lobular, multiseptated, and hyperintense signal covering the whole lesion. Ultrasound evaluation can also be useful in the differentiation of ganglion cysts from other soft tissue lesions [13, 14]. In the present report, we only used MRI for diagnosis.
Treatment of ganglion cysts includes a conservative approach or surgical intervention. In symptomatic cases, surgical excision is the treatment of choice. Also, in cases with atypical localization, difficult needle aspiration, and a high risk of recurrence, surgical resection is recommended. Post-excision recurrence may occur due to the inadequate resection of the tumor mass.
Although atypical localization of ganglion cysts rarely occurs, it should be considered in the differential diagnosis of hand and wrist lesions. In our case, the growth speed and clinical course did not raise the clinical suspicion of malignancy. However, due to the proximity of the mass in the thenar area and its proximity to the crucial adjacent structures, including the recurrent branch of the median nerve and digital nerve, early and accurate diagnosis and treatment through timely clinical investigation and complete preoperative imaging analysis are required.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research and considering that the article is a case report and that the university has not defined a code of ethics for this type of article, the research has been done with the patient's consent at all stages.
Funding
The article is the result of the author's research at the Bone and Joint Research Center of Shafaihiyaian Hospital, Iran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
- Wang AA, Hutchinson DT. Longitudinal observation of pediatric hand and wrist ganglia. J Hand Surg Am. 2001; 26(4):599-602. [DOI:10.1053/jhsu.2001.26141] [PMID]
- Shahryar Kamrani R, Oryadi Zanjani L, Nabian MH. Arthroscopic curettage of intraosseous ganglions of the lunate bone. J Res Orthop Sci. 2014; 1(4). [Link]
- Dehghani H, Khadem M, Bahari M. Elbow region ganglion cyst: A case report and brief review of literature. J Res Orthop Scie. 2020; 7(2):87-92. [DOI:10.32598/JROSJ.7.2.619.1]
- Shariatzade H, Barkam M, Saied A, Akbarzadeh Arab A. Scapholunate instability following the surgical excision of dorsal ganglion cyst of the wrist: A case report. J Res Orthop Sci. 2021; 8(2):95-100. [DOI:10.32598/JROSJ.8.2.723.2]
- Gude W, Morelli V. Ganglion cysts of the wrist: Pathophysiology, clinical picture, and management. Curr Rev Musculoskelet Med. 2008; 1(3-4):205-11. [DOI:10.1007/s12178-008-9033-4] [PMID] [PMCID]
- Nahra ME, Bucchieri JS. Ganglion cysts and other tumor related conditions of the hand and wrist. Hand Clin. 2004; 20(3):249-60. [DOI:10.1016/j.hcl.2004.03.015] [PMID]
- Khubaib MU, Monaco R. Unique location and origin of a ganglion cyst. Cureus. 2021; 13(7):e16453. [DOI:10.7759/cureus.16453]
- Mirzaei A, Joharimoghadam MM, Zabihiyeganeh M. Adalimumab-Responsive refractory sarcoidosis following multiple eyebrow tattoos: A case report. Tanaffos. 2017; 16(1):80-3. [PMID]
- Jamshidi K, Mirzaei A, Bagherifard A, Bahrabadi M. Rare case of small size Extraskeletal Ewing Sarcoma arising from the median nerve with paresthesia. J Orthop Sci. 2018; 23(2):430-2. [DOI:10.1016/j.jos.2016.07.017] [PMID]
- Thornburg LE. Ganglions of the hand and wrist. J Am Acad Orthop Surg. 1999; 7(4):231-8. [DOI:10.5435/00124635-199907000-00003] [PMID]
- Chiu DT, Ascherman JA. An intramuscular ganglion presenting as a thenar mass. Plast Reconstr Surg. 1994; 93(3):606-7. [DOI:10.1097/00006534-199493030-00029]
- Azzopardi EA, Gujral S, Mandal A, Kulkarni M. Rapidly expanding thenar eminence ganglion: A case report. Cases J. 2009; 2:129. [DOI:10.1186/1757-1626-2-129] [PMID] [PMCID]
- AbiEzzi SS, Miller LS. The use of ultrasound for the diagnosis of soft-tissue masses in children. J Pediatr Orthop. 1995; 15(5):566-73. [DOI:10.1097/01241398-199509000-00003] [PMID]
- Neto N, Nunnes P. Spectrum of MRI features of ganglion and synovial cysts. Insights Imaging. 2016; 7(2):179-86. [DOI:10.1007/s13244-016-0463-z] [PMID] [PMCID]
Type of Study: Case Report |
Subject:
Hand surgery / Elbow
Received: 2022/08/31 | Accepted: 2022/12/1 | Published: 2022/05/1
Received: 2022/08/31 | Accepted: 2022/12/1 | Published: 2022/05/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
