

Volume 9, Issue 3 (8-2022)
JROS 2022, 9(3): 157-164 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ebrahimpour A, Biglari F, Sabaghzadeh A, Barazandeh Rad S, Sadighi M, Moradian T et al . Comparing the Effects of Vitamins C and D in Preventing Complex Regional Pain Syndrome After Distal Radius Fracture Treatment. JROS 2022; 9 (3) :157-164
URL: http://jros.iums.ac.ir/article-1-2221-en.html
URL: http://jros.iums.ac.ir/article-1-2221-en.html
Adel Ebrahimpour1 

 , Farsad Biglari1 , Amir Sabaghzadeh1 , Saber Barazandeh Rad1 , Mehrdad Sadighi1 , Tohid Moradian1 , Meisam Jafari Kafiabadi1
, Farsad Biglari1 , Amir Sabaghzadeh1 , Saber Barazandeh Rad1 , Mehrdad Sadighi1 , Tohid Moradian1 , Meisam Jafari Kafiabadi1
, Farsad Biglari1 , Amir Sabaghzadeh1 , Saber Barazandeh Rad1 , Mehrdad Sadighi1 , Tohid Moradian1 , Meisam Jafari Kafiabadi1
1- Department of Orthopedic Surgery, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 721 kb]
(518 Downloads)
| Abstract (HTML) (1589 Views)
Full-Text: (542 Views)
1. Introduction
Complex regional pain syndrome (CRPS) also known as reflex sympathetic dystrophy is a chronic pain condition that most commonly affects individuals after trauma and injury [1]. The prevalence of CPRS after distal radius fractures is different in studies ranging from 1% to 27%, with a predilection for the female gender [2, 3]. The exact pathophysiology of CRPS is unknown but current evidence suggests that a nerve injury, inflammation, and immune system play a role in the occurrence of CRPS [4]. CRPS can be categorized into two types: Type I, characterized by CRPS without evident nerve injury, and type II, resulting from nerve injury. CRPS type I is associated with severe pain, adversely affecting the patient’s psychosocial well-being and daily functioning [5].
Notably, numerous studies have pointed to the involvement of oxygen-free radicals in the pathogenesis of CRPS. Consequently, the administration of free radical scavengers may have the potential to prevent the occurrence of this syndrome. Some studies suggest that vitamin C administration can limit soft tissue damage and prevent CRPS type I [6]. Similarly, vitamin D is known for its anti-inflammatory properties. This vitamin plays a role in regulating muscle function, inflammation, and the immune system. A study has also shown that low vitamin D levels are associated with an increased likelihood of developing CPRS I [7].
The primary aim of this study was to compare the effectiveness of vitamins C and D in preventing the occurrence of CRPS following the fixation of distal radius fractures. By shedding light on the potential benefits of these vitamins in reducing CRPS incidence, this research seeks to contribute to improved patient outcomes and reduced healthcare costs associated with this debilitating condition.
2. Methods
The study design was a double-blind, randomized clinical trial conducted from January 1, 2018, to the end of December 2019. Inclusion criteria were as follows: Individuals with distal radius fractures between the ages of 18 and 65 years, those indicated for distal radius fracture fixation using external fixators and the PCP method, written consent for intervention and participation in the study, and the ability to take vitamins C and D orally. Exclusion criteria were applied to avoid confounding factors, and patients meeting any of the following criteria were excluded from the study: Those already taking vitamin D or other vitamin supplements or osteoporosis medications at the time of injury, individuals with medical conditions affecting vitamin D levels, those unwilling to participate in the study, patients with other fractures, neuropathy, or open fractures, and those with serious pre-existing medical conditions that could influence the study’s results, such as ischemic heart disease, stroke, diabetes mellitus, hypertension, hypothyroidism, and rheumatoid arthritis.
The sampling method was continuous sampling. The sample size was calculated using the following formula considering the type I error of 5% and power of 80%. After confirming the inclusion and exclusion criteria, a total of 150 participants were allocated into three groups as follows:
A) The first group received a daily prescription of 500 mg of vitamin C for 50 days.
B) The second group received an oral dose of 5000 IU of vitamin D weekly for 6 weeks.
C) The third group served as the control group and did not receive any form of complementary medicine.
After the surgery, patients were discharged from the hospital on the following day, and the range of motion exercises commenced immediately. After six weeks, the outpatients had the pins and external fixator removed and were subsequently scheduled for follow-up visits at 2, 6, and 12 weeks. Physiotherapy sessions began immediately after the second surgery, which involved pin and external fixator removal. At the study’s outset, as well as during subsequent visits and at the time of discharge, all relevant information was meticulously recorded using a checklist specifically designed for each group. Following the surgical procedures, patients were evaluated for CRPS symptoms at the 6th and 12th weeks post-surgery. In case of any suspicion of CRPS, further monitoring was conducted in the 6th and 12th months. The CRPS improvement process in patients was also closely evaluated.
To assess comparability between the treatment and control groups concerning patient characteristics and prognostic measures at baseline, the chi-square, independent sample t-test, or Mann–Whitney test was utilized as appropriate. Data are presented as Mean±SD or percentages, as applicable. Logistic regression analysis using the forward conditional method was performed to estimate the predictive value of the included variables on the occurrence of CRPS type I. Statistical significance was set at P≤0.05. All statistical analyses were conducted using SPSS software, version 21 (SPSS, Inc., Chicago, IL, USA).
3. Results
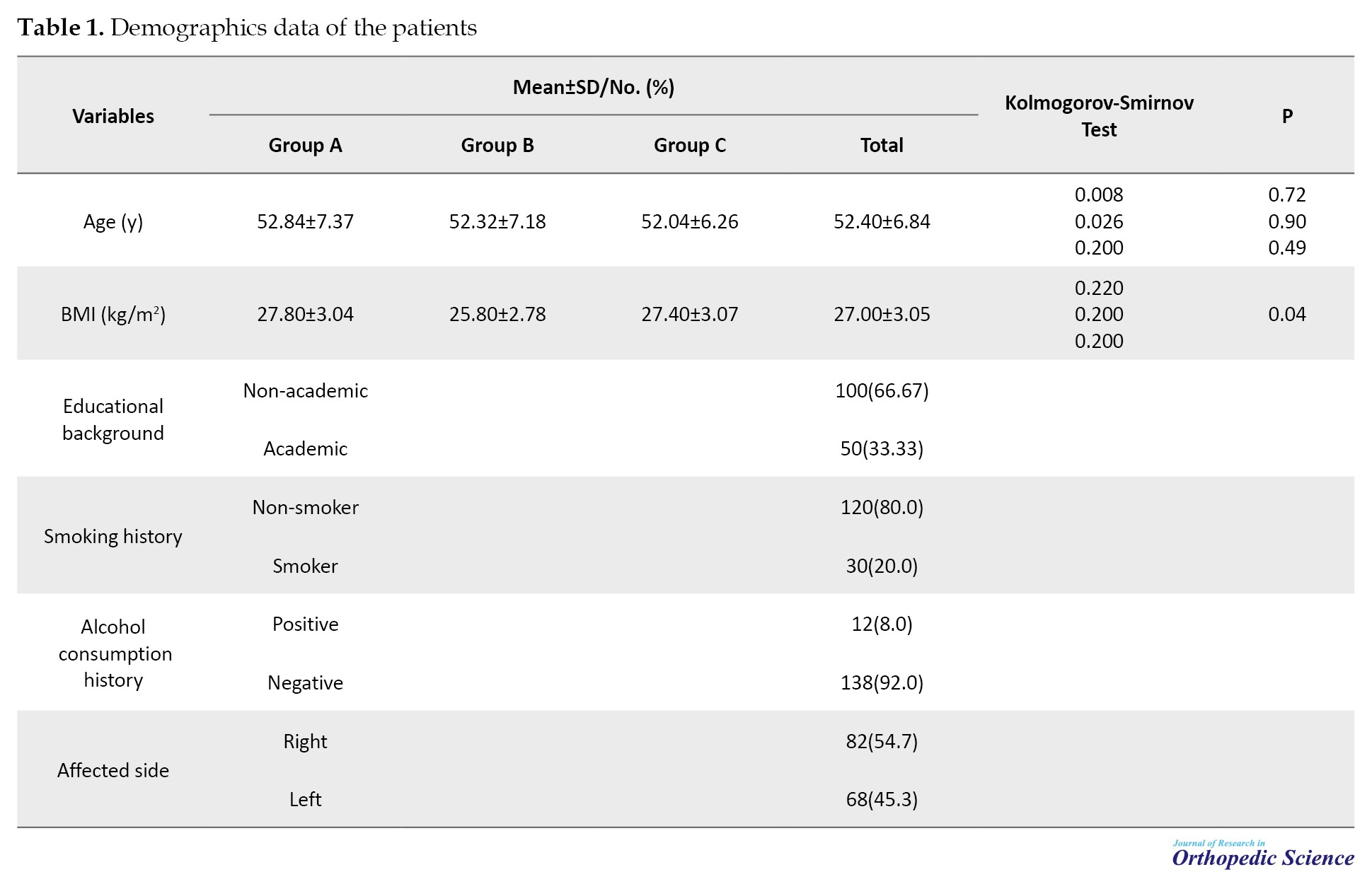
The mean age of the patients was 52.40±6.84 years and did not differ significantly among the three study groups. The mean body mass index (BMI) of the patients was 27.00±3.05 kg/m2. Regarding educational background, 100 cases (66.67%) had a non-academic education, while 50 cases (33.33%) had an academic education.
Upon arrival, participants were asked about their history of smoking and alcohol consumption. Among the total participants, 30 cases (20.0%) had a history of smoking, and 12 cases (8.0%) had a history of alcohol consumption. Importantly, all individuals who reported a history of alcohol consumption were also smokers. The distribution of distal radius fractures among the patients showed that 82 patients (54.7%) had fractures in the right hand, while 68 patients (45.3%) had fractures in the left hand. The leading cause of trauma among the patients was falling (Table 1).
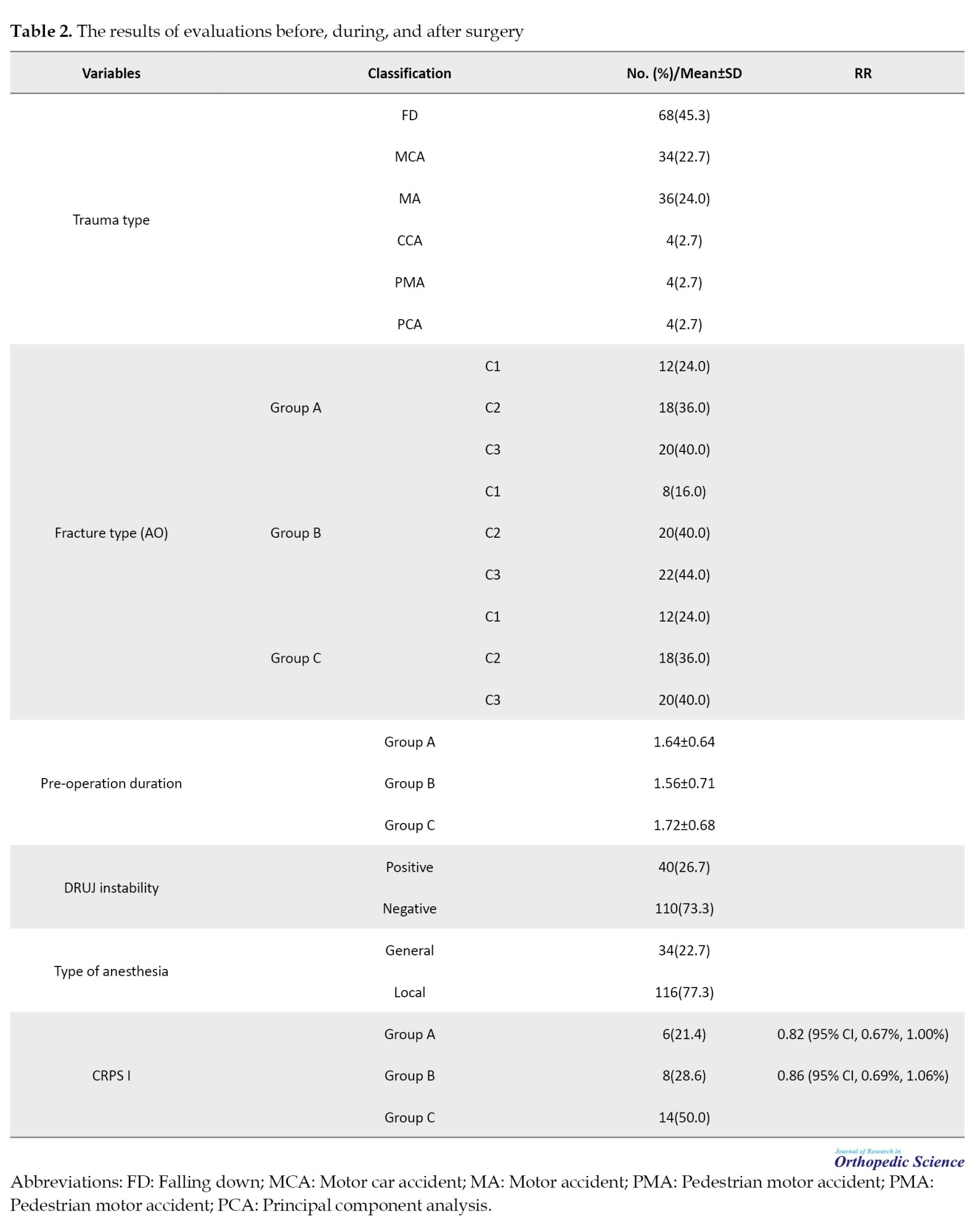
According to the AO/OTA classification, all participants experienced distal radius fractures of type C, with the majority falling into categories C2 and C3. Among the 150 fractures, 62 patients were classified as type C3, 56 patients as type C2, and 32 patients as type C1 (Figure 1).
 The mean pre-operation duration from fracture to surgery in the participants was 1.64±0.67 days, and the groups showed similarity in this aspect. Similarly, the mean duration of surgery was 1.25±0.15 hours, with no significant differences observed between the groups.
The mean pre-operation duration from fracture to surgery in the participants was 1.64±0.67 days, and the groups showed similarity in this aspect. Similarly, the mean duration of surgery was 1.25±0.15 hours, with no significant differences observed between the groups.
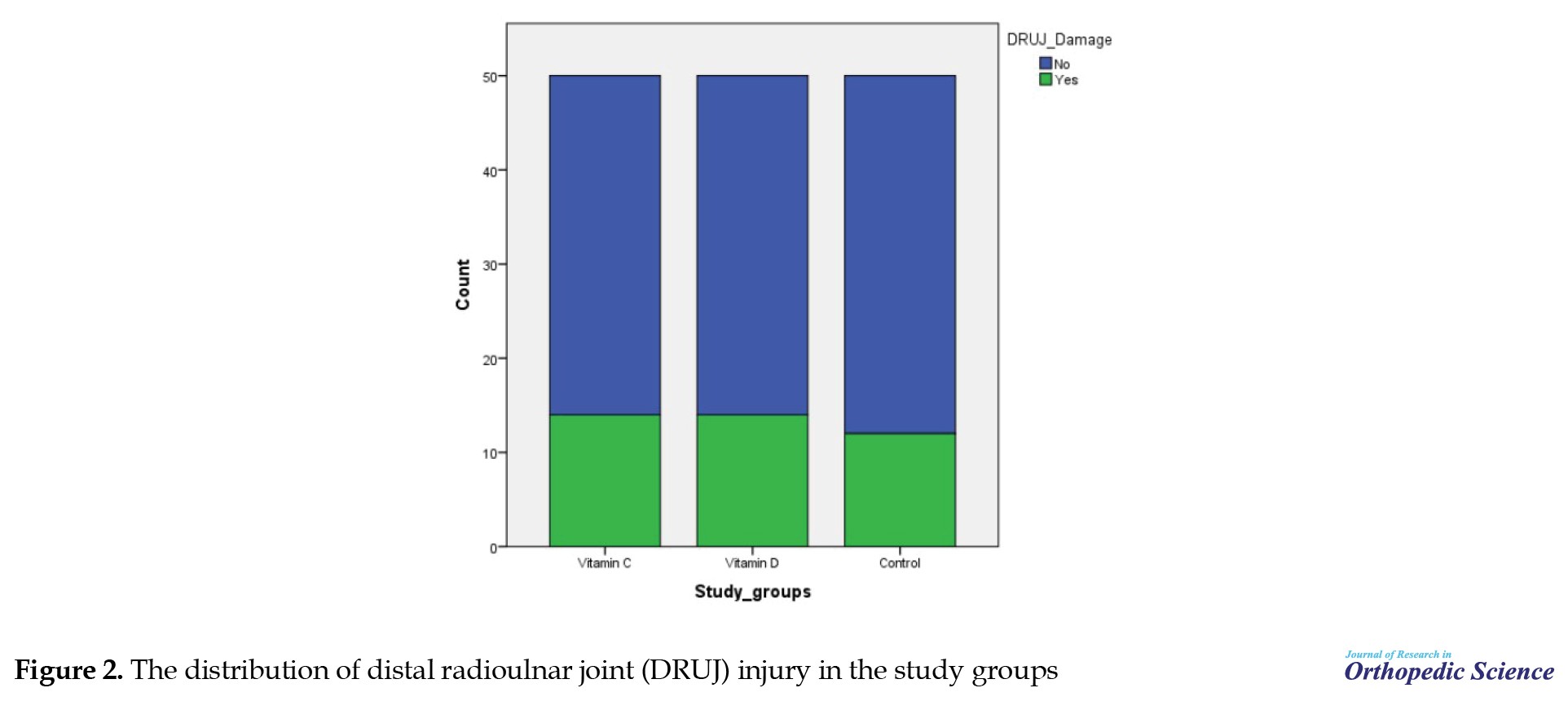
Participants received either general or local anesthesia based on their conditions. Out of the 150 study participants, 34 patients (22.7%) underwent general anesthesia, while 116 patients (77.3%) received local anesthesia. Additionally, the presence of DRUJ instability was assessed. Among the 150 patients, 40 cases (26.7%) showed DRUJ instability, while 110 patients (73.3%) had no DRUJ damage (Figure 2).
 Notably, all patients with DRUJ injury, in addition to the external fixator and DRUJ pin, also underwent long arm splinting.
Notably, all patients with DRUJ injury, in addition to the external fixator and DRUJ pin, also underwent long arm splinting.
During the follow-up visit, CRPS occurred in 28 patients (18.7%), of whom 14 patients (50%) belonged to group C, 8 patients (28.6%) belonged to group B, and 6 patients (21.4%) belonged to group A (Figure 3).
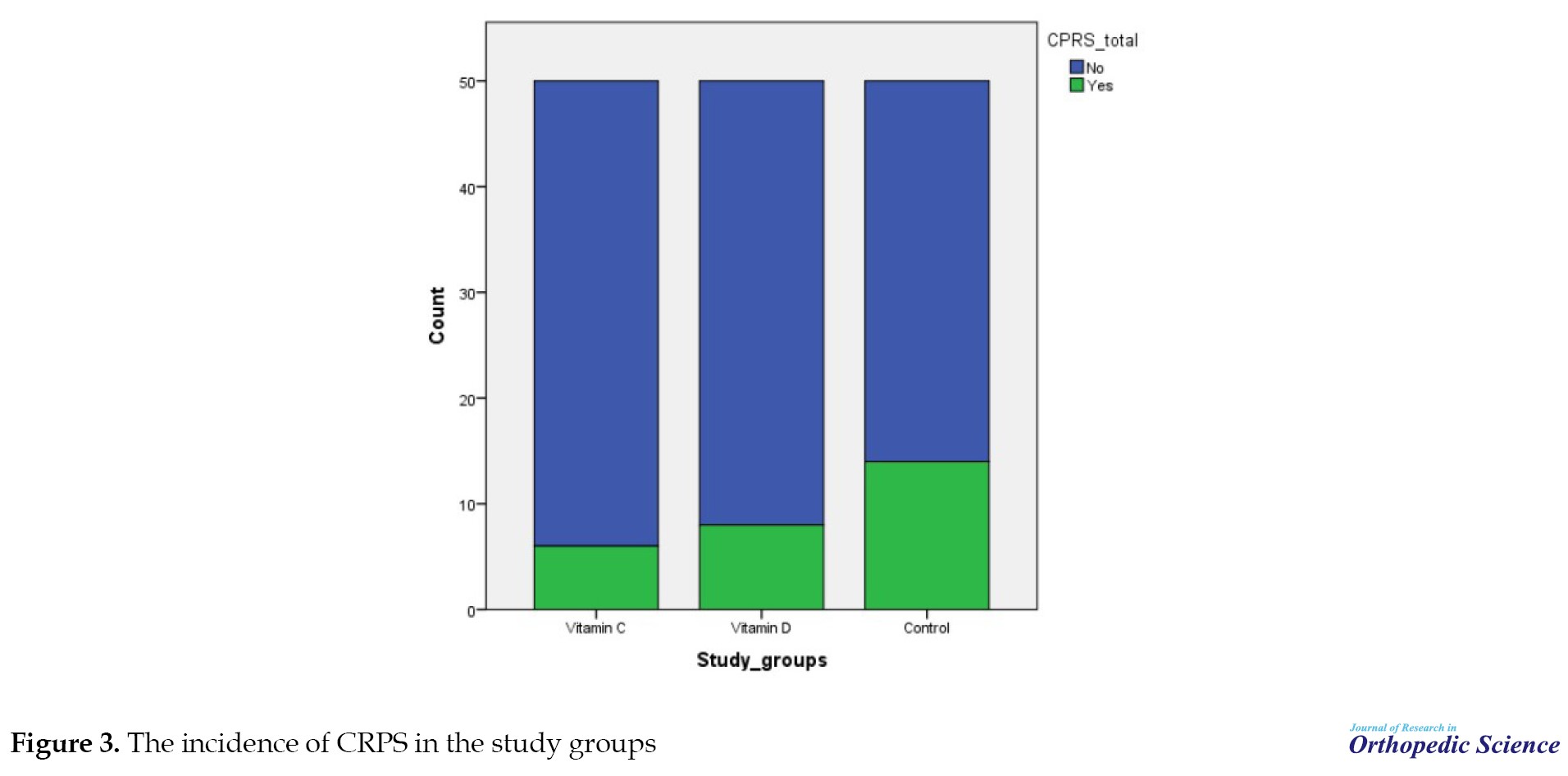 When comparing groups A and B to group C, the relative risk was calculated for each. The risk value obtained for the consumption of vitamin C compared to the control group was 0.82 (95% CI, 0.67%, 1.00%). Therefore, vitamin C consumption reduces the risk of CRPS by 18% compared to not consuming vitamin C, and this reduction is approaching statistical significance.
When comparing groups A and B to group C, the relative risk was calculated for each. The risk value obtained for the consumption of vitamin C compared to the control group was 0.82 (95% CI, 0.67%, 1.00%). Therefore, vitamin C consumption reduces the risk of CRPS by 18% compared to not consuming vitamin C, and this reduction is approaching statistical significance.
On the other hand, the risk value obtained for the consumption of vitamin D compared to group C was 0.86 (95% CI, 0.69%, 1.06%). Thus, the use of vitamin D reduces the risk of CRPS by 14% compared to not using vitamin D; however, this reduction did not reach a statistically significant level (Table 2).
4. Discussion
Numerous studies have explored the effects of vitamins C and D in preventing and treating CRPS; however, our study stands out as the first to directly compare the effectiveness of these vitamins in preventing CRPS after a distal radius fracture. While Lee et al. researched the impact of vitamin D on CRPS incidence with a comparable number of participants, it is essential to note that their focus was on different types of distal radius fractures and diverse treatment approaches [7]. In contrast, in our study, all patients had type C fractures and underwent the same surgical procedure.
The study conducted by Alimian et al. considered the effect of topical vitamin C in Bier’s block during the initial stage of fracture on CRPS occurrence after surgery for distal radius fractures [6]. It should be noted that the indication for surgery in those patients was entirely different from our study. Additionally, unlike our study, topical vitamin C was used as an adjuvant for Bier’s block in addition to its systemic distribution. Similar to our findings, the study reported a reduction in CRPS occurrence with the use of vitamin C, estimating a 15% reduction in risk [6]. In our study, vitamin C intake resulted in a reduction in CRPS risk compared to the controls, and this reduction was close to the threshold of statistical significance. Furthermore, our study examined the trend related to vitamin C in reducing CRPS symptoms, which was not investigated in this study.
Ekrol et al. investigated the effect of vitamin C on functional outcomes after distal radius fractures [8]. Although they included distal radius fracture patients and divided them into groups receiving 500 mg of vitamin C daily or a placebo for 50 days after surgery, in contrast to our study, their results showed no difference in the incidence of CRPS among the study groups.
Zollinger et al. performed a study in the Netherlands in 2010 to evaluate the effect of three different doses of vitamin C on the occurrence of CRPS type I [9]. The doses of vitamin C were randomly assigned to different treatment groups, and no relationship was observed between vitamin C and external fixator use in the occurrence of CRPS. However, this study did not investigate the simultaneous effect of external fixator and vitamin C, leaving uncertainty about the effect of each intervention separately.
Several systematic reviews and meta-analyses have been conducted in this area. Meena et al. investigated the effect of vitamin C on the occurrence of CRPS and concluded that its use, even with diverse doses, leads to a significant reduction in the incidence of CRPS [10]. However, they recommended further studies and larger meta-analyses with more valid questionnaires to strengthen the evidence.
A literature review by Malay and Chung in 2016 aimed to examine the validity of the recommendation to receive vitamin C for preventing CRPS in patients with distal radius fractures [11]. The study indicated a small reduction in CRPS risk but highlighted the need for criteria, such as biological logic, specificity, and coherence to be met. The researchers were not entirely certain about the effect of vitamin C and suggested more studies with higher power to conclude [11].
Our study has several limitations, including the absence of a placebo in the control group, the lack of serum vitamin D level measurements, and a relatively small number of cases, which may limit the generalizability of the findings. However, despite these limitations, our research provides valuable insights into the comparative effectiveness of vitamins C and D in preventing CRPS after distal radius fracture. To further bolster the evidence and draw more definitive conclusions, future studies with larger sample sizes and rigorous methodologies are warranted.
5. Conclusion
In conclusion, our study demonstrated that both vitamins C and D were effective in reducing the incidence of CRPS in patients with distal radius fractures. Additionally, vitamin C proved to be significantly beneficial in improving CRPS symptoms, reducing pain, and alleviating limitations in range of motion. However, further clinical trial studies with larger and more diverse populations are essential to gain a deeper understanding of this topic and to validate our findings.
Declarations
There is no conflict of interest to declare.
Data availability statement
The Data supporting the findings of this study are available upon request from the corresponding author and with permission from Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Ethical Considerations
Compliance with ethical guidelines
This study (trial code: 64190) was registered on the Iranian Registry of Clinical Trials (IRCT) (Code: IRCT20211201053235N6).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Meisam Jafari Kafiabadi; Data acquisition: Amir Sabaghzadeh, Saber Barazandeh Rad and Mehrdad Sadighi; Data analysis: Tohid Moradian, and Farsad Biglari; Review, editing and final approval: Meisam Jafari Kafiabadi, and Adel Ebrahimpour.
Conflict of interest
The authors declared no conflicts of interests.
References
Complex regional pain syndrome (CRPS) also known as reflex sympathetic dystrophy is a chronic pain condition that most commonly affects individuals after trauma and injury [1]. The prevalence of CPRS after distal radius fractures is different in studies ranging from 1% to 27%, with a predilection for the female gender [2, 3]. The exact pathophysiology of CRPS is unknown but current evidence suggests that a nerve injury, inflammation, and immune system play a role in the occurrence of CRPS [4]. CRPS can be categorized into two types: Type I, characterized by CRPS without evident nerve injury, and type II, resulting from nerve injury. CRPS type I is associated with severe pain, adversely affecting the patient’s psychosocial well-being and daily functioning [5].
Notably, numerous studies have pointed to the involvement of oxygen-free radicals in the pathogenesis of CRPS. Consequently, the administration of free radical scavengers may have the potential to prevent the occurrence of this syndrome. Some studies suggest that vitamin C administration can limit soft tissue damage and prevent CRPS type I [6]. Similarly, vitamin D is known for its anti-inflammatory properties. This vitamin plays a role in regulating muscle function, inflammation, and the immune system. A study has also shown that low vitamin D levels are associated with an increased likelihood of developing CPRS I [7].
The primary aim of this study was to compare the effectiveness of vitamins C and D in preventing the occurrence of CRPS following the fixation of distal radius fractures. By shedding light on the potential benefits of these vitamins in reducing CRPS incidence, this research seeks to contribute to improved patient outcomes and reduced healthcare costs associated with this debilitating condition.
2. Methods
The study design was a double-blind, randomized clinical trial conducted from January 1, 2018, to the end of December 2019. Inclusion criteria were as follows: Individuals with distal radius fractures between the ages of 18 and 65 years, those indicated for distal radius fracture fixation using external fixators and the PCP method, written consent for intervention and participation in the study, and the ability to take vitamins C and D orally. Exclusion criteria were applied to avoid confounding factors, and patients meeting any of the following criteria were excluded from the study: Those already taking vitamin D or other vitamin supplements or osteoporosis medications at the time of injury, individuals with medical conditions affecting vitamin D levels, those unwilling to participate in the study, patients with other fractures, neuropathy, or open fractures, and those with serious pre-existing medical conditions that could influence the study’s results, such as ischemic heart disease, stroke, diabetes mellitus, hypertension, hypothyroidism, and rheumatoid arthritis.
The sampling method was continuous sampling. The sample size was calculated using the following formula considering the type I error of 5% and power of 80%. After confirming the inclusion and exclusion criteria, a total of 150 participants were allocated into three groups as follows:
A) The first group received a daily prescription of 500 mg of vitamin C for 50 days.
B) The second group received an oral dose of 5000 IU of vitamin D weekly for 6 weeks.
C) The third group served as the control group and did not receive any form of complementary medicine.
After the surgery, patients were discharged from the hospital on the following day, and the range of motion exercises commenced immediately. After six weeks, the outpatients had the pins and external fixator removed and were subsequently scheduled for follow-up visits at 2, 6, and 12 weeks. Physiotherapy sessions began immediately after the second surgery, which involved pin and external fixator removal. At the study’s outset, as well as during subsequent visits and at the time of discharge, all relevant information was meticulously recorded using a checklist specifically designed for each group. Following the surgical procedures, patients were evaluated for CRPS symptoms at the 6th and 12th weeks post-surgery. In case of any suspicion of CRPS, further monitoring was conducted in the 6th and 12th months. The CRPS improvement process in patients was also closely evaluated.
To assess comparability between the treatment and control groups concerning patient characteristics and prognostic measures at baseline, the chi-square, independent sample t-test, or Mann–Whitney test was utilized as appropriate. Data are presented as Mean±SD or percentages, as applicable. Logistic regression analysis using the forward conditional method was performed to estimate the predictive value of the included variables on the occurrence of CRPS type I. Statistical significance was set at P≤0.05. All statistical analyses were conducted using SPSS software, version 21 (SPSS, Inc., Chicago, IL, USA).
3. Results
The mean age of the patients was 52.40±6.84 years and did not differ significantly among the three study groups. The mean body mass index (BMI) of the patients was 27.00±3.05 kg/m2. Regarding educational background, 100 cases (66.67%) had a non-academic education, while 50 cases (33.33%) had an academic education.
Upon arrival, participants were asked about their history of smoking and alcohol consumption. Among the total participants, 30 cases (20.0%) had a history of smoking, and 12 cases (8.0%) had a history of alcohol consumption. Importantly, all individuals who reported a history of alcohol consumption were also smokers. The distribution of distal radius fractures among the patients showed that 82 patients (54.7%) had fractures in the right hand, while 68 patients (45.3%) had fractures in the left hand. The leading cause of trauma among the patients was falling (Table 1).
According to the AO/OTA classification, all participants experienced distal radius fractures of type C, with the majority falling into categories C2 and C3. Among the 150 fractures, 62 patients were classified as type C3, 56 patients as type C2, and 32 patients as type C1 (Figure 1).
Participants received either general or local anesthesia based on their conditions. Out of the 150 study participants, 34 patients (22.7%) underwent general anesthesia, while 116 patients (77.3%) received local anesthesia. Additionally, the presence of DRUJ instability was assessed. Among the 150 patients, 40 cases (26.7%) showed DRUJ instability, while 110 patients (73.3%) had no DRUJ damage (Figure 2).
During the follow-up visit, CRPS occurred in 28 patients (18.7%), of whom 14 patients (50%) belonged to group C, 8 patients (28.6%) belonged to group B, and 6 patients (21.4%) belonged to group A (Figure 3).
On the other hand, the risk value obtained for the consumption of vitamin D compared to group C was 0.86 (95% CI, 0.69%, 1.06%). Thus, the use of vitamin D reduces the risk of CRPS by 14% compared to not using vitamin D; however, this reduction did not reach a statistically significant level (Table 2).
4. Discussion
Numerous studies have explored the effects of vitamins C and D in preventing and treating CRPS; however, our study stands out as the first to directly compare the effectiveness of these vitamins in preventing CRPS after a distal radius fracture. While Lee et al. researched the impact of vitamin D on CRPS incidence with a comparable number of participants, it is essential to note that their focus was on different types of distal radius fractures and diverse treatment approaches [7]. In contrast, in our study, all patients had type C fractures and underwent the same surgical procedure.
The study conducted by Alimian et al. considered the effect of topical vitamin C in Bier’s block during the initial stage of fracture on CRPS occurrence after surgery for distal radius fractures [6]. It should be noted that the indication for surgery in those patients was entirely different from our study. Additionally, unlike our study, topical vitamin C was used as an adjuvant for Bier’s block in addition to its systemic distribution. Similar to our findings, the study reported a reduction in CRPS occurrence with the use of vitamin C, estimating a 15% reduction in risk [6]. In our study, vitamin C intake resulted in a reduction in CRPS risk compared to the controls, and this reduction was close to the threshold of statistical significance. Furthermore, our study examined the trend related to vitamin C in reducing CRPS symptoms, which was not investigated in this study.
Ekrol et al. investigated the effect of vitamin C on functional outcomes after distal radius fractures [8]. Although they included distal radius fracture patients and divided them into groups receiving 500 mg of vitamin C daily or a placebo for 50 days after surgery, in contrast to our study, their results showed no difference in the incidence of CRPS among the study groups.
Zollinger et al. performed a study in the Netherlands in 2010 to evaluate the effect of three different doses of vitamin C on the occurrence of CRPS type I [9]. The doses of vitamin C were randomly assigned to different treatment groups, and no relationship was observed between vitamin C and external fixator use in the occurrence of CRPS. However, this study did not investigate the simultaneous effect of external fixator and vitamin C, leaving uncertainty about the effect of each intervention separately.
Several systematic reviews and meta-analyses have been conducted in this area. Meena et al. investigated the effect of vitamin C on the occurrence of CRPS and concluded that its use, even with diverse doses, leads to a significant reduction in the incidence of CRPS [10]. However, they recommended further studies and larger meta-analyses with more valid questionnaires to strengthen the evidence.
A literature review by Malay and Chung in 2016 aimed to examine the validity of the recommendation to receive vitamin C for preventing CRPS in patients with distal radius fractures [11]. The study indicated a small reduction in CRPS risk but highlighted the need for criteria, such as biological logic, specificity, and coherence to be met. The researchers were not entirely certain about the effect of vitamin C and suggested more studies with higher power to conclude [11].
Our study has several limitations, including the absence of a placebo in the control group, the lack of serum vitamin D level measurements, and a relatively small number of cases, which may limit the generalizability of the findings. However, despite these limitations, our research provides valuable insights into the comparative effectiveness of vitamins C and D in preventing CRPS after distal radius fracture. To further bolster the evidence and draw more definitive conclusions, future studies with larger sample sizes and rigorous methodologies are warranted.
5. Conclusion
In conclusion, our study demonstrated that both vitamins C and D were effective in reducing the incidence of CRPS in patients with distal radius fractures. Additionally, vitamin C proved to be significantly beneficial in improving CRPS symptoms, reducing pain, and alleviating limitations in range of motion. However, further clinical trial studies with larger and more diverse populations are essential to gain a deeper understanding of this topic and to validate our findings.
Declarations
There is no conflict of interest to declare.
Data availability statement
The Data supporting the findings of this study are available upon request from the corresponding author and with permission from Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Ethical Considerations
Compliance with ethical guidelines
This study (trial code: 64190) was registered on the Iranian Registry of Clinical Trials (IRCT) (Code: IRCT20211201053235N6).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Meisam Jafari Kafiabadi; Data acquisition: Amir Sabaghzadeh, Saber Barazandeh Rad and Mehrdad Sadighi; Data analysis: Tohid Moradian, and Farsad Biglari; Review, editing and final approval: Meisam Jafari Kafiabadi, and Adel Ebrahimpour.
Conflict of interest
The authors declared no conflicts of interests.
References
- Bruehl S. Complex Regional Pain syndrome. BMJ. 2015; 351:h2730. [DOI:10.1136/bmj.h2730] [PMID]
- Beerthuizen A, Stronks DL, Van't Spijker A, Yaksh A, Hanraets BM, Klein J, et al. Demographic and medical parameters in the development of Complex Regional Pain syndrome type 1 (CRPS1): Prospective study on 596 patients with a fracture. Pain. 2012; 153(6):1187-92. [DOI:10.1016/j.pain.2012.01.026] [PMID]
- de Mos M, de Bruijn AG, Huygen FJ, Dieleman JP, Stricker BH, Sturkenboom MC. The incidence of Complex Regional Pain syndrome: A population-based study. Pain. 2007; 129(1-2):12-20. [DOI:10.1016/j.pain.2006.09.008] [PMID]
- Dey S, Guthmiller KB, Varacallo M. Complex Regional Pain syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. [PMID]
- Galer BS, Henderson J, Perander J, Jensen MP. Course of symptoms and quality of life measurement in Complex Regional Pain syndrome: A pilot survey. J Pain Symptom Manage. 2000; 20(4):286-92. [DOI:10.1016/S0885-3924(00)00183-4] [PMID]
- Alimian M, Sobhani Eraghi A, Chavoshizadeh SA, Mohseni M, Mousavi E, Movassaghi S. Regional vitamin C in bier block reduces the incidence of CRPS-1 following distal radius fracture surgery. Eur J Orthop Surg Traumatol. 2021; 31(4):689-93. [DOI:10.1007/s00590-020-02821-0] [PMID]
- Lee SU, Na KT, Lee YM, Park JH, Joo SY. Low vitamin D levels in post-menopausal women are associated with Complex Regional Pain syndrome type I in surgically treated distal radius fractures. J Orthop Surg Res. 2020; 15(1):328. [DOI:10.1186/s13018-020-01859-4] [PMID]
- Ekrol I, Duckworth AD, Ralston SH, Court-Brown CM, McQueen MM. The influence of vitamin C on the outcome of distal radial fractures: A double-blind, randomized controlled trial. J Bone Joint Surg Am. 2014; 96(17):1451-9. [DOI:10.2106/JBJS.M.00268] [PMID]
- Zollinger PE, Kreis RW, van der Meulen HG, van der Elst M, Breederveld RS, Tuinebreijer WE. No higher risk of CRPS after external fixation of distal radial fractures - Subgroup analysis under randomised vitamin C prophylaxis. Open Orthop J. 2010; 4:71-5. [DOI:10.2174/1874325001004020071] [PMID]
- Meena S, Sharma P, Gangary SK, Chowdhury B. Role of vitamin C in prevention of Complex Regional Pain syndrome after distal radius fractures: A meta-analysis. Eur J Orthop Surg Traumatol. 2015; 25(4):637-41. [DOI:10.1007/s00590-014-1573-2] [PMID]
- Malay S, Chung KC. Testing the validity of preventing Chronic Regional Pain syndrome with vitamin C after distal radius fracture. [Corrected]. J Hand Surg Am. 2014; 39(11):2251-7. [DOI:10.1016/j.jhsa.2014.08.009] [PMID]
Type of Study: Research Article |
Subject:
Trauma
Received: 2022/02/12 | Accepted: 2022/03/28 | Published: 2022/08/1
Received: 2022/02/12 | Accepted: 2022/03/28 | Published: 2022/08/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
