

Volume 9, Issue 4 (11-2022)
JROS 2022, 9(4): 201-208 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nabian M H, komijani M, Sharafi M H, Shayan-Moghadam R, Mehrabi Y, Babaei Nejad E. Comparing Conventional C-arm and Navigation Methods for Distal Küntscher Screw Insertion in Femur and Tibia Fractures. JROS 2022; 9 (4) :201-208
URL: http://jros.iums.ac.ir/article-1-2229-en.html
URL: http://jros.iums.ac.ir/article-1-2229-en.html
Mohammad Hossein Nabian1 

 , Mehdi Komijani1 , Mohammad Hasan Sharafi1 , Ramin Shayan-Moghadam1 , Yosef Mehrabi1 , Erfan Babaei Nejad 1
, Mehdi Komijani1 , Mohammad Hasan Sharafi1 , Ramin Shayan-Moghadam1 , Yosef Mehrabi1 , Erfan Babaei Nejad 1
, Mehdi Komijani1 , Mohammad Hasan Sharafi1 , Ramin Shayan-Moghadam1 , Yosef Mehrabi1 , Erfan Babaei Nejad 1
1- Department of Orthopedic and Trauma Surgery, School of Medicine, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
Keywords: Orthopedics, Fracture of the long bones of the lower limb, Intramedullary nail (IMN), Navigation, Distal locking screw
Full-Text [PDF 2034 kb]
(105 Downloads)
| Abstract (HTML) (417 Views)
Full-Text: (107 Views)
1. Introduction
Intramedullary nail (IMN) usage is one of the main proposed methods in fixing long bone fractures [1]. These nails are locked in the proximal and distal using screws to prevent rotational movements and shortening of the broken limb [2]. Proximal screw implantation often employs specialized jigs that can easily insert the screw in the proximal part [3]. This method is used for screw placement due to the curvature of the bone canal or bending of the nail when it is placed in the canal [4].
Distal nail screw implantation is associated with many errors [5]. Two methods exist for distal nail screw insertion [6]. The first method involves mechanical jigs, known as the conventional method, while the other method employs the freehand technique under fluoroscopic guidance [7]. The latter entails tilting the C-arm towards the direction of the distal locking holes and the screw is placed by manually placing the drill in the direction of the distal holes under fluoroscopic repetition [8]. However, both methods are associated with increased procedure time, radiation exposure, and screw misalignment, primarily due to jig accuracy [9]. Given these limitations, it is imperative to explore alternative methods.
C-arm-based navigation integrates surgical actions with medical imaging, aiming to mitigate radiation exposure, shortening the surgical duration, and improving accuracy [10]. This method allows screw insertion without repeated imaging. For this purpose, the position of the surgical instruments, the patient’s bone, and the contour are determined in the three-dimensional space with the help of tracking systems. Also, the relation of C-arm images with 3D space is determined through a calibration process. By combining this information, the position of the tools about the patient is displayed on the images. In other words, the view shown to the surgeon will be the same as fluoroscopy images, with the difference that these images are provided virtually and without radiation [11].
This study aims to facilitate the insertion of the distal femoral and tibia nail screw by comparing the conventional C-arm method and the C-arm-based navigation method in patients with femur or tibia fractures. Our goal was to identify a method that reduce the duration of the surgery, and the amount of radiation received by the patient, the surgeon, and the operating room staff and also diminished the error in the distal femur and tibia nail screw surgery.
2. Methods
This clinical trial involved 44 patients with fractures of the long bones of the lower limb (femur shaft or tibia) referred to Shariati Hospital who are candidates for IMN implantation. All patients voluntarily participated in this research and were given the necessary information before filling out the questionnaire. Completing the questionnaires was considered consent to participate in the study. The questionnaires were filled anonymously and the participants’ information was kept completely confidential (this study has been approved by the Institutional Review Board of Tehran University of Medical Sciences, Tehran, Iran).
Patients with an open fracture of the femur or tibia shaft, small canal diameter, osseous canal obstruction, and a history of infection or active infection of the osseous canal were excluded from the study. Participants were randomly and equally divided into control and intervention groups. The control group underwent distal femur or tibia screw placement using the conventional C-arm method, while the intervention group received screw insertion using the C-arm-based navigation method. Demographic information of patients, including age, gender, weight, type and severity of the fracture, and underlying diseases of patients was extracted from the patient medical file. During surgery, several parameters, including the duration of surgery were examined. It was calculated from the start until the completion of distal nail screw insertion. The duration of surgery was accurately measured and recorded using a timer by a person outside the operation room. Another parameter to be investigated was the radiation time given by the C-arm device. It was measured from the default settings of the C-arm device. Also, the number of attempts to insert the distal nail screws was recorded by a person outside the operation team. The number of repetitions of the screw insertion and the number of times of drilling the distal screw location until achieving the best possible result were recorded.
Insertion of distal Kuntscher screws by c-arm-based navigation method
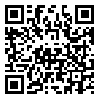
After placing the nail in the intervention group and starting the process of distal screw insertion, first, the frame was installed on the C-arm (Figure 1).
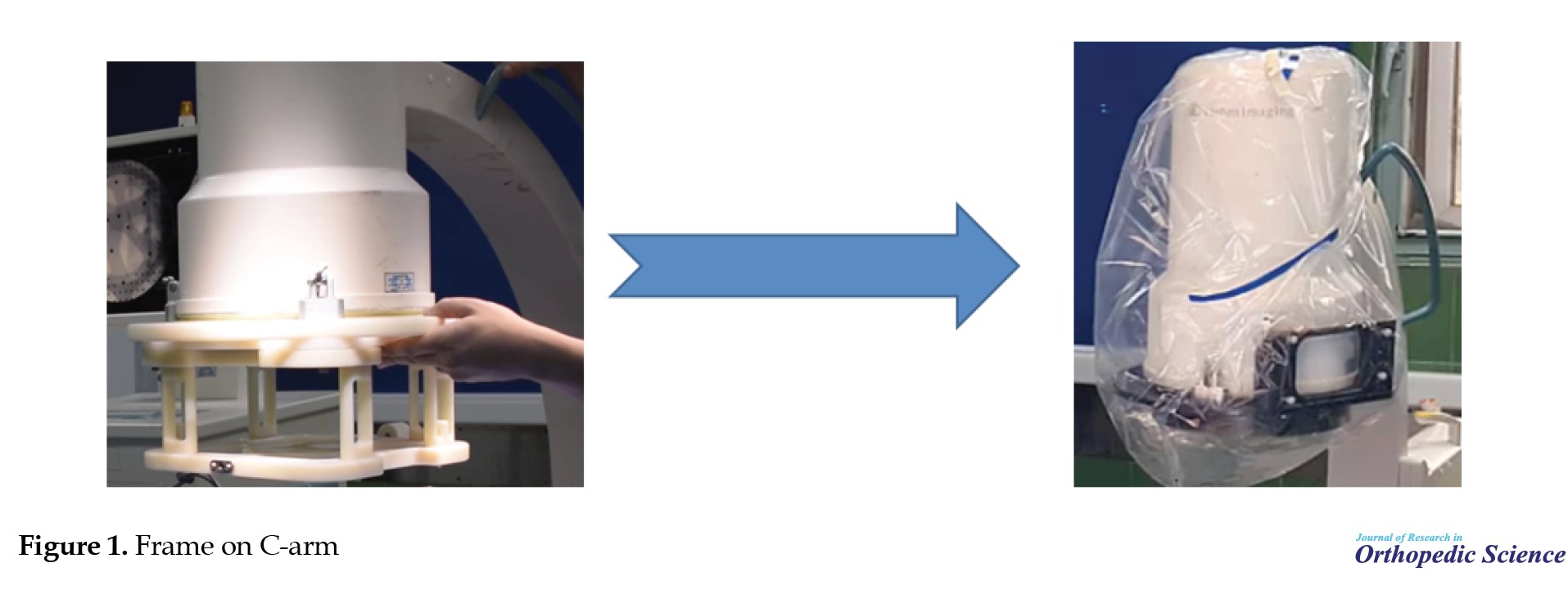 Antero-posterior (AP) and lateral images were taken from the distal Kuntscher and screw holes. The AP and lateral images should be consistent with the location of the screws. Therefore, the shape of the screw holes should be circular in the graph (Figure 2).
Antero-posterior (AP) and lateral images were taken from the distal Kuntscher and screw holes. The AP and lateral images should be consistent with the location of the screws. Therefore, the shape of the screw holes should be circular in the graph (Figure 2).
 To check the three-dimensional position of the Kuntscher holes, balls were installed on the C-arm frame that could be seen by the camera. The sample of the primary frame was large. Therefore, a frame with a smaller volume and a more favorable material was designed.
To check the three-dimensional position of the Kuntscher holes, balls were installed on the C-arm frame that could be seen by the camera. The sample of the primary frame was large. Therefore, a frame with a smaller volume and a more favorable material was designed.
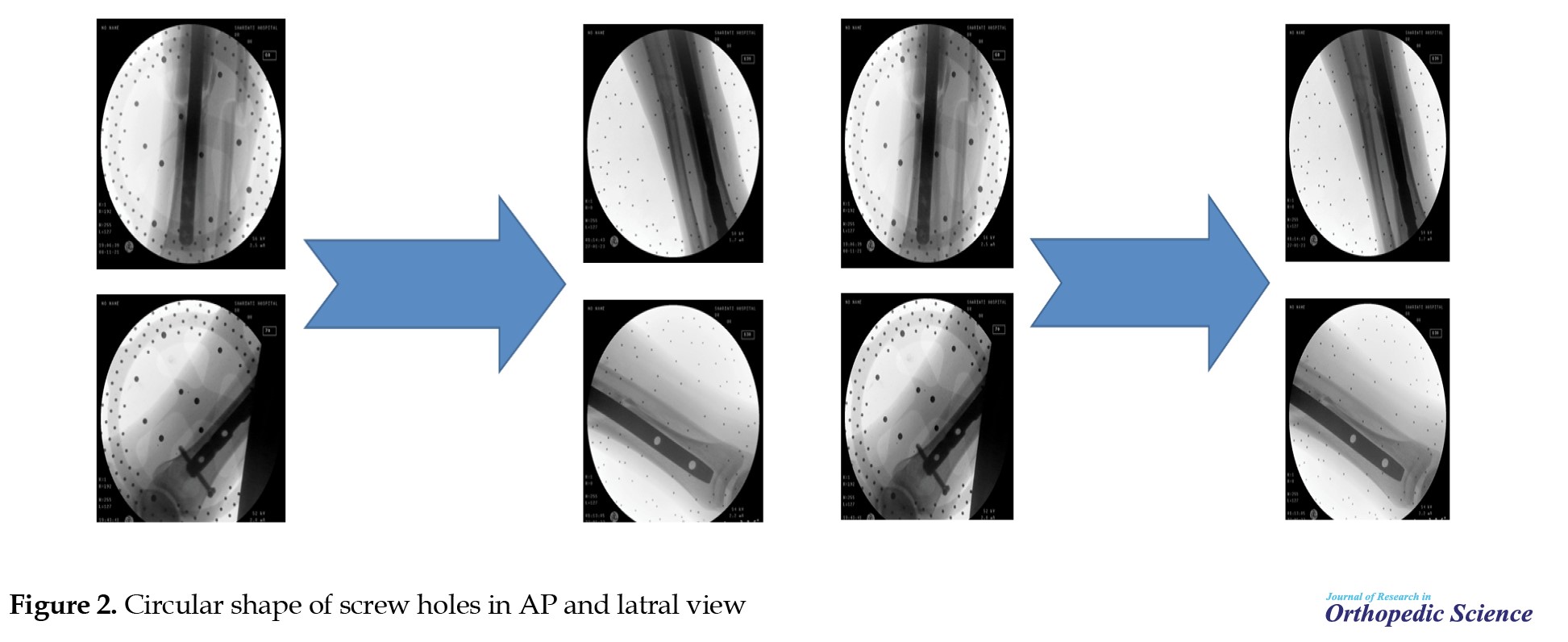
In this navigation system, there were three reference numbers defined by silver spheres. The first reference was placed on the C-arm frame, the second or central reference was placed on the Kuntscher to maintain the position of the Kuntscher and not to lose alignment by changing the foot position, and the third reference was placed on the drill or guide when drilling the bone (Figure 3).
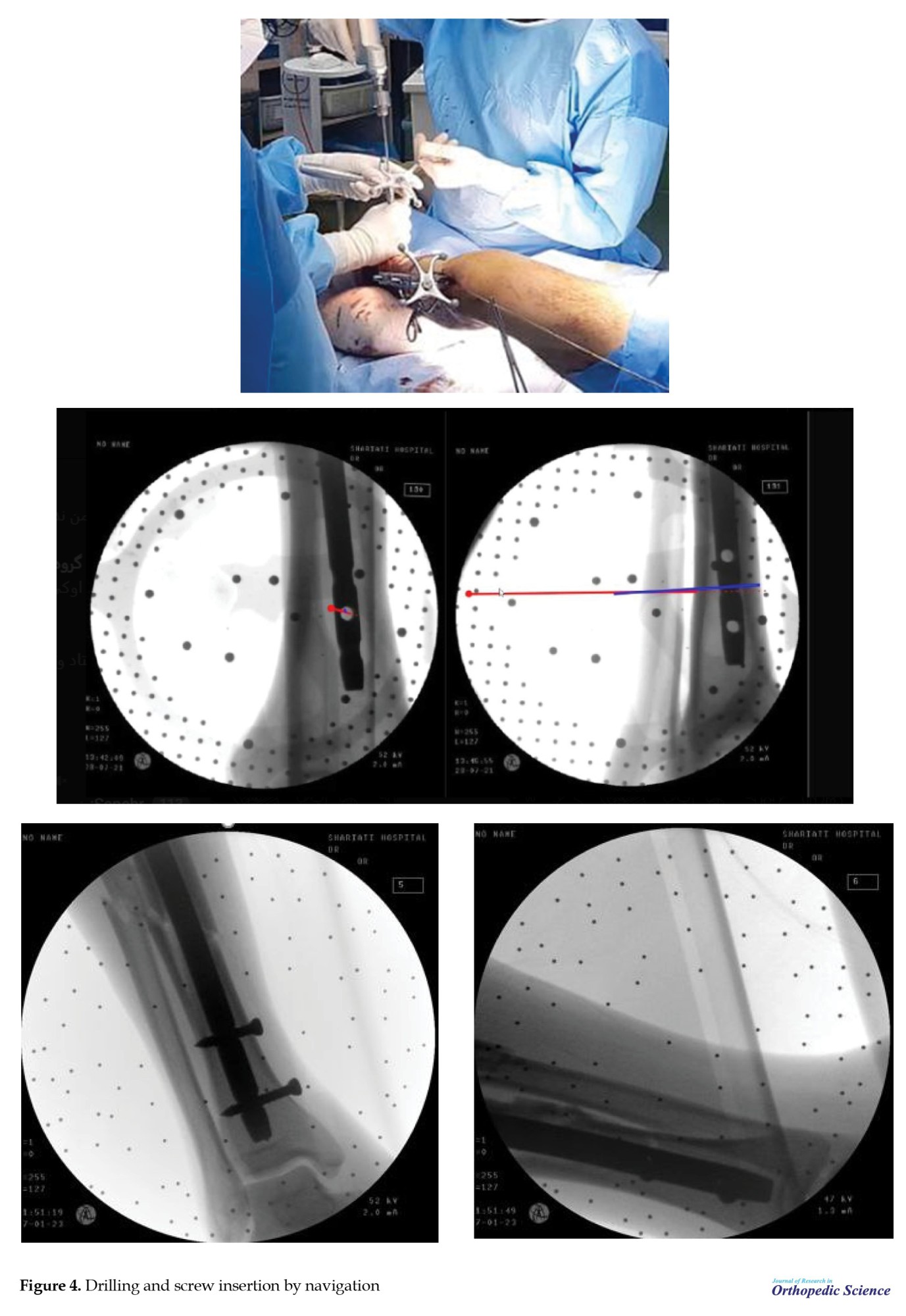
 After preparing the AP and lateral graphs and using the references, the alignment of the drill and the third reference was calibrated and the screw insertion was done by navigation method (Figure 4).
After preparing the AP and lateral graphs and using the references, the alignment of the drill and the third reference was calibrated and the screw insertion was done by navigation method (Figure 4).
Sample size calculation
A sample size of 44 patients (22 in each group) was determined to detect a meaningful difference of half an hour in surgery duration between groups, with a power of 90% and a type 1 error of 5%.
Statistical analysis
Data were reported as Mean±SD or median (25th-75th interquartile range) for quantitative variables and number (percentage) for qualitative variables. Baseline characteristics were compared between groups using the chi-square test, Fisher’s exact test, Mann-Whitney U test, or independent sample t-test, depending on the nature of the data. The significance level was set at P<0.05. Statistical analysis was performed using SPSS software, version 25.
3. Results
As shown in Figure 5, distal nail screw insertion was done for 22 patients in the control group by the conventional method and 22 patients in the intervention group by the navigation method.
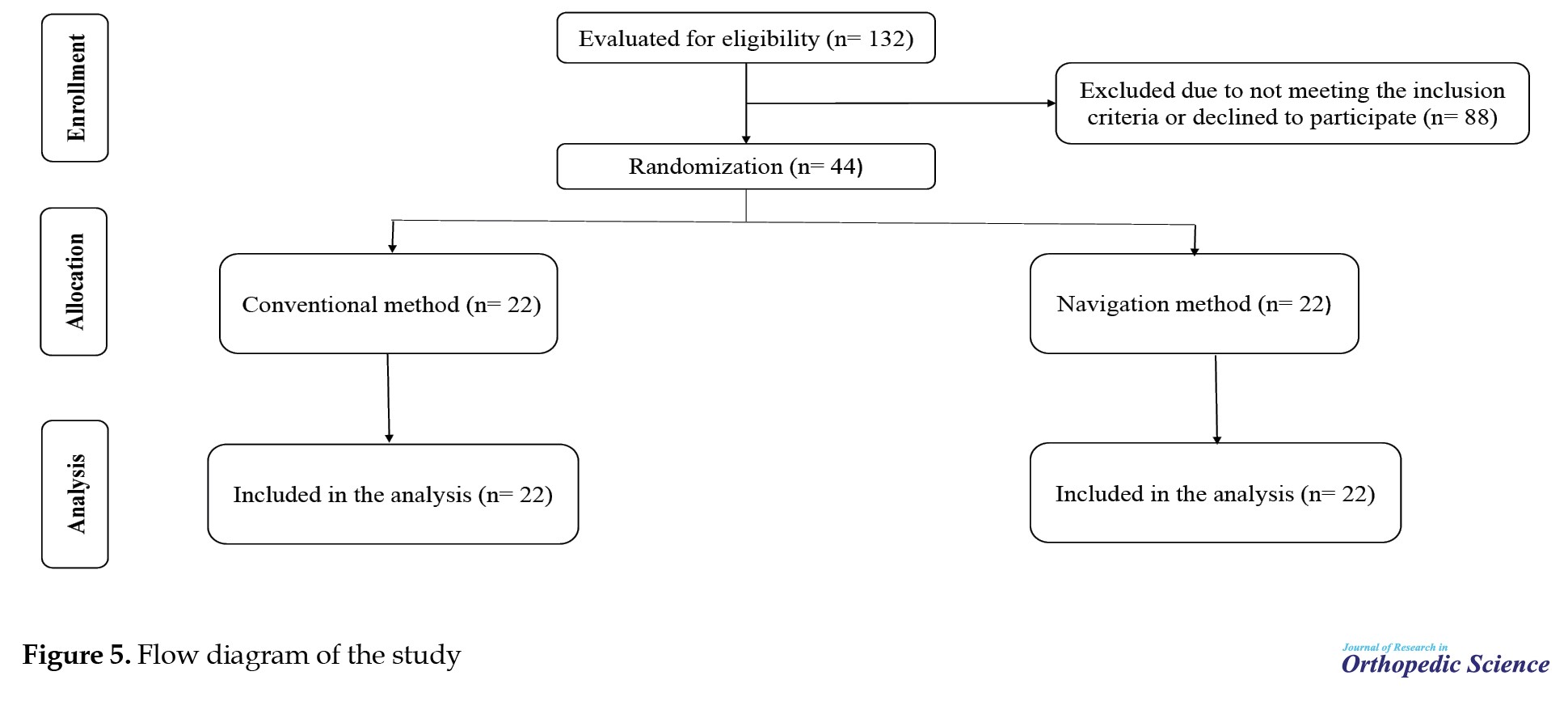 A total of 38 and 23 screws were successfully placed in the control and intervention groups, respectively. The success rate was calculated as the ratio of the number of screws that have been successfully applied to the total number of screws. Table 1 presents the baseline characteristics of study participants.
A total of 38 and 23 screws were successfully placed in the control and intervention groups, respectively. The success rate was calculated as the ratio of the number of screws that have been successfully applied to the total number of screws. Table 1 presents the baseline characteristics of study participants.
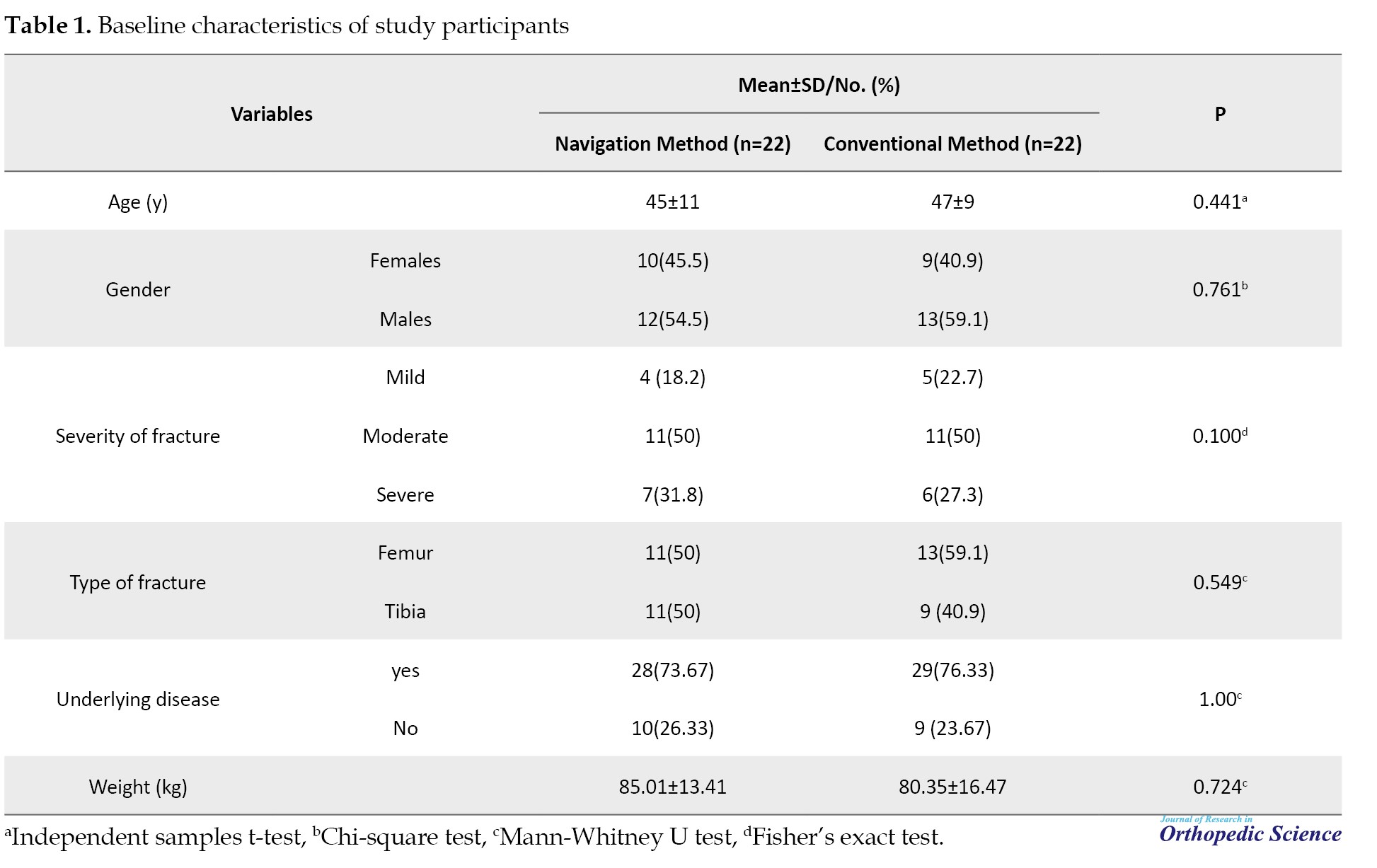
No significant difference was observed in terms of age, gender, weight, type and severity of fractures, and underlying diseases among participants. As demonstrated in Table 2, the percentage of success in insertion of nail screws in the control and intervention groups was 77% and 65%, respectively.

Although the percentage of success in the intervention group is lower, this difference is not statistically significant (P=0.36). The number of attempts for successful screw insertion was also similar in two groups. Table 3 presents the number of radiation exposures to observe the position of the screws in the intervention and control groups.
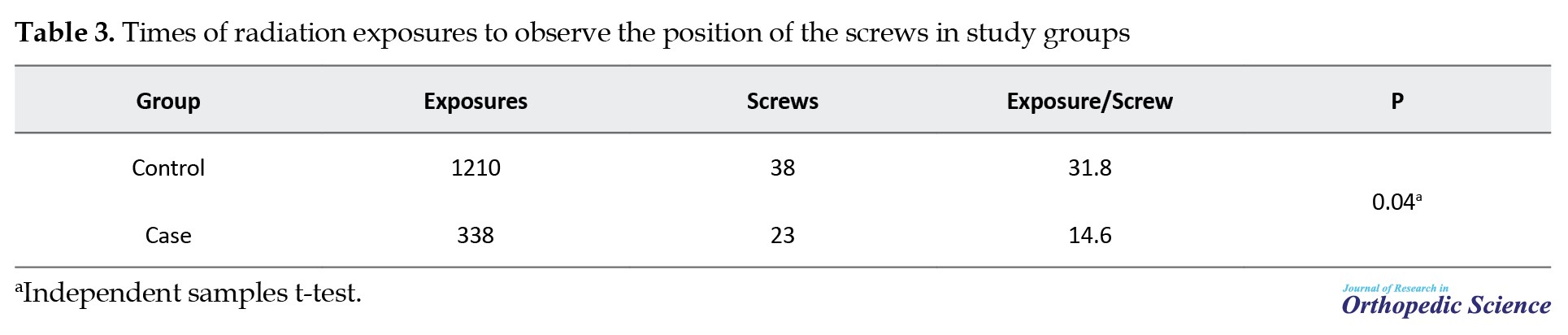
For each successful screw in the control and intervention groups, radiation was given 31 and 14 times. A significant reduction was observed in using x-rays for screw insertion by C-arm based navigation method (P=0.04). As disclosed in Table 4, the time spent for screw placement in the control group was 17 hours and 6 minutes for 38 screws, indicating that about 26 minutes were needed for each successful screw placement.
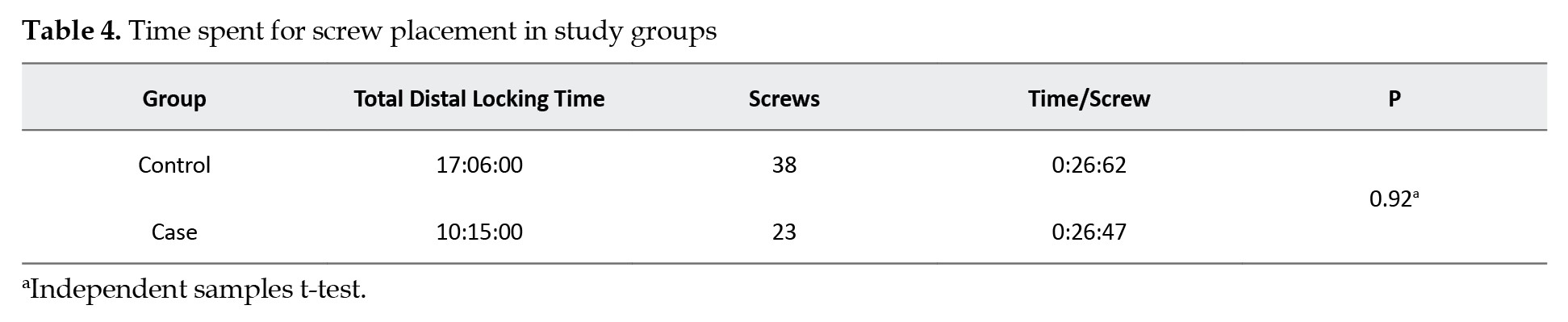
On the other hand, the total time of screw insertion in the case group was 10 hours and 15 minutes for 23 screws. In other words, it took about 26 minutes to insert each successful screw in the intervention group. No significant difference was observed between study groups in the duration of screw insertion (P=0.92).
4. Discussion
According to our knowledge, the present study is the first to compare the consequences of the conventional C-arm method and C-arm-based navigation method for distal Kuntscher screw insertion in fractures of the long bones of the lower limb in patients with the femur or tibia fractures. Our main results indicate that while the success rate and duration of distal nail screw insertion were almost similar between the two methods, the use of C-arm-based navigation significantly reduced radiation exposure repetition.
In a study conducted by Guo et al. [12], 37 patients in the control group underwent free-hand pedicle screw placement and 37 patients in the case group underwent pedicle screw placement with the help of navigation. In contrast with our results, the mentioned study was in favor of the navigation method and showed that the success rate in screw placement was 94.6% in the case group and 70.27% in the control group [12]. Also, in a study by Elmi-Terander et al. [13], a significant increase in accuracy of screw insertion by navigation method was detected. In this study, the accuracy of pedicle screw placement in the case group that underwent the augmented reality surgical navigation method was 93.9% and in the control group that underwent fluoroscopy-assisted free-hand surgery was 89.6% [13].
Regarding radiation exposure, consistent with our results, Guo et al [12] showed that in the pedicle screw insertion by navigation method, the radiation exposure times were significantly reduced compared to the free-hand method. Moreover, in a study conducted on 10 lower limbs prepared from cadavers, it was shown that in the distal leg nail screws insertion, the times of radiation exposure for each screw were reduced by 58%, which was significantly less than the conventional method [9]. In addition, Hawi et al [14] compared the consequences of distal femoral nail screw insertion using by navigation method and conventional method. This study showed that the radiation exposure times in the navigation method were significantly reduced compared to the conventional method [14]. Furthermore, in a study conducted on 42 patients with distal nail locking screw insertion, the average times of radiation exposure were reduced in the control group (screw insertion without using the navigation method) compared to the intervention group (screw insertion using the navigation method). However, the duration of screw insertion was shorter in the control group [15].
Regarding the duration of surgery and screw insertion, in contrast with our results, a study by Elmi-Terander et al. [13] found a non-significant increase in the duration of pedicle screw insertion by the navigation-assisted method. Also, another study disclosed that the duration of distal femoral nail screws insertion by the navigation method was significantly more than the conventional method [14]. However, according to the conclusion of another research, a significant decrease was observed in the duration of screwing for pedicle screw insertion by the navigation method compared to the free-hand method [12]. Additionally, for nail screw insertion, a significant decrease (22%) in the duration of operation and screw insertion was observed in the navigation method compared to the conventional method [9].
The discrepancies between our results and the mentioned results may be caused by the different nature and design of the studies and their various populations.
5. Conclusion
The use of navigation as a new technology in orthopedics may have a significant impact on the process of distal IMN screw insertion. Although the accuracy of both methods was almost the same, the navigation method reduces the frequency and times of radiation exposure for screw placement. Further well-designed studies with greater sample sizes are required to clarify and compare the consequences of the conventional C-arm method and C-arm-based navigation method for distal Kuntcher screw insertion in patients with the femur or tibia fractures.
Study strengths and limitations
The present investigation has several strengths, including comparing consequences of the conventional C-arm method and C-arm-based navigation method for distal Kuntcher screw insertion in fractures of the long bones of the lower limb, for the first time. Also, appropriate sample size and robust statistical analysis can be considered other strengths. However, connecting and stabilizing the reference to the Kuntcher, the placement space of the calibration frame, sterilizing various parts, and communication with radiographic systems are among the most critical limitations of the present study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran University of Medical Sciences.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Mohammad Hosein Nabian; Methodology: Mehdi Komijanii; Data collection, investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all the surgeons, medical staff, and research team members who contributed to this study. The authors also thank their patients for their participation and trust. Special thanks to Tehran University of Medical Sciences for providing support and resources throughout the research process.
References
Intramedullary nail (IMN) usage is one of the main proposed methods in fixing long bone fractures [1]. These nails are locked in the proximal and distal using screws to prevent rotational movements and shortening of the broken limb [2]. Proximal screw implantation often employs specialized jigs that can easily insert the screw in the proximal part [3]. This method is used for screw placement due to the curvature of the bone canal or bending of the nail when it is placed in the canal [4].
Distal nail screw implantation is associated with many errors [5]. Two methods exist for distal nail screw insertion [6]. The first method involves mechanical jigs, known as the conventional method, while the other method employs the freehand technique under fluoroscopic guidance [7]. The latter entails tilting the C-arm towards the direction of the distal locking holes and the screw is placed by manually placing the drill in the direction of the distal holes under fluoroscopic repetition [8]. However, both methods are associated with increased procedure time, radiation exposure, and screw misalignment, primarily due to jig accuracy [9]. Given these limitations, it is imperative to explore alternative methods.
C-arm-based navigation integrates surgical actions with medical imaging, aiming to mitigate radiation exposure, shortening the surgical duration, and improving accuracy [10]. This method allows screw insertion without repeated imaging. For this purpose, the position of the surgical instruments, the patient’s bone, and the contour are determined in the three-dimensional space with the help of tracking systems. Also, the relation of C-arm images with 3D space is determined through a calibration process. By combining this information, the position of the tools about the patient is displayed on the images. In other words, the view shown to the surgeon will be the same as fluoroscopy images, with the difference that these images are provided virtually and without radiation [11].
This study aims to facilitate the insertion of the distal femoral and tibia nail screw by comparing the conventional C-arm method and the C-arm-based navigation method in patients with femur or tibia fractures. Our goal was to identify a method that reduce the duration of the surgery, and the amount of radiation received by the patient, the surgeon, and the operating room staff and also diminished the error in the distal femur and tibia nail screw surgery.
2. Methods
This clinical trial involved 44 patients with fractures of the long bones of the lower limb (femur shaft or tibia) referred to Shariati Hospital who are candidates for IMN implantation. All patients voluntarily participated in this research and were given the necessary information before filling out the questionnaire. Completing the questionnaires was considered consent to participate in the study. The questionnaires were filled anonymously and the participants’ information was kept completely confidential (this study has been approved by the Institutional Review Board of Tehran University of Medical Sciences, Tehran, Iran).
Patients with an open fracture of the femur or tibia shaft, small canal diameter, osseous canal obstruction, and a history of infection or active infection of the osseous canal were excluded from the study. Participants were randomly and equally divided into control and intervention groups. The control group underwent distal femur or tibia screw placement using the conventional C-arm method, while the intervention group received screw insertion using the C-arm-based navigation method. Demographic information of patients, including age, gender, weight, type and severity of the fracture, and underlying diseases of patients was extracted from the patient medical file. During surgery, several parameters, including the duration of surgery were examined. It was calculated from the start until the completion of distal nail screw insertion. The duration of surgery was accurately measured and recorded using a timer by a person outside the operation room. Another parameter to be investigated was the radiation time given by the C-arm device. It was measured from the default settings of the C-arm device. Also, the number of attempts to insert the distal nail screws was recorded by a person outside the operation team. The number of repetitions of the screw insertion and the number of times of drilling the distal screw location until achieving the best possible result were recorded.
Insertion of distal Kuntscher screws by c-arm-based navigation method
After placing the nail in the intervention group and starting the process of distal screw insertion, first, the frame was installed on the C-arm (Figure 1).
In this navigation system, there were three reference numbers defined by silver spheres. The first reference was placed on the C-arm frame, the second or central reference was placed on the Kuntscher to maintain the position of the Kuntscher and not to lose alignment by changing the foot position, and the third reference was placed on the drill or guide when drilling the bone (Figure 3).
Sample size calculation
A sample size of 44 patients (22 in each group) was determined to detect a meaningful difference of half an hour in surgery duration between groups, with a power of 90% and a type 1 error of 5%.
Statistical analysis
Data were reported as Mean±SD or median (25th-75th interquartile range) for quantitative variables and number (percentage) for qualitative variables. Baseline characteristics were compared between groups using the chi-square test, Fisher’s exact test, Mann-Whitney U test, or independent sample t-test, depending on the nature of the data. The significance level was set at P<0.05. Statistical analysis was performed using SPSS software, version 25.
3. Results
As shown in Figure 5, distal nail screw insertion was done for 22 patients in the control group by the conventional method and 22 patients in the intervention group by the navigation method.
No significant difference was observed in terms of age, gender, weight, type and severity of fractures, and underlying diseases among participants. As demonstrated in Table 2, the percentage of success in insertion of nail screws in the control and intervention groups was 77% and 65%, respectively.
Although the percentage of success in the intervention group is lower, this difference is not statistically significant (P=0.36). The number of attempts for successful screw insertion was also similar in two groups. Table 3 presents the number of radiation exposures to observe the position of the screws in the intervention and control groups.
For each successful screw in the control and intervention groups, radiation was given 31 and 14 times. A significant reduction was observed in using x-rays for screw insertion by C-arm based navigation method (P=0.04). As disclosed in Table 4, the time spent for screw placement in the control group was 17 hours and 6 minutes for 38 screws, indicating that about 26 minutes were needed for each successful screw placement.
On the other hand, the total time of screw insertion in the case group was 10 hours and 15 minutes for 23 screws. In other words, it took about 26 minutes to insert each successful screw in the intervention group. No significant difference was observed between study groups in the duration of screw insertion (P=0.92).
4. Discussion
According to our knowledge, the present study is the first to compare the consequences of the conventional C-arm method and C-arm-based navigation method for distal Kuntscher screw insertion in fractures of the long bones of the lower limb in patients with the femur or tibia fractures. Our main results indicate that while the success rate and duration of distal nail screw insertion were almost similar between the two methods, the use of C-arm-based navigation significantly reduced radiation exposure repetition.
In a study conducted by Guo et al. [12], 37 patients in the control group underwent free-hand pedicle screw placement and 37 patients in the case group underwent pedicle screw placement with the help of navigation. In contrast with our results, the mentioned study was in favor of the navigation method and showed that the success rate in screw placement was 94.6% in the case group and 70.27% in the control group [12]. Also, in a study by Elmi-Terander et al. [13], a significant increase in accuracy of screw insertion by navigation method was detected. In this study, the accuracy of pedicle screw placement in the case group that underwent the augmented reality surgical navigation method was 93.9% and in the control group that underwent fluoroscopy-assisted free-hand surgery was 89.6% [13].
Regarding radiation exposure, consistent with our results, Guo et al [12] showed that in the pedicle screw insertion by navigation method, the radiation exposure times were significantly reduced compared to the free-hand method. Moreover, in a study conducted on 10 lower limbs prepared from cadavers, it was shown that in the distal leg nail screws insertion, the times of radiation exposure for each screw were reduced by 58%, which was significantly less than the conventional method [9]. In addition, Hawi et al [14] compared the consequences of distal femoral nail screw insertion using by navigation method and conventional method. This study showed that the radiation exposure times in the navigation method were significantly reduced compared to the conventional method [14]. Furthermore, in a study conducted on 42 patients with distal nail locking screw insertion, the average times of radiation exposure were reduced in the control group (screw insertion without using the navigation method) compared to the intervention group (screw insertion using the navigation method). However, the duration of screw insertion was shorter in the control group [15].
Regarding the duration of surgery and screw insertion, in contrast with our results, a study by Elmi-Terander et al. [13] found a non-significant increase in the duration of pedicle screw insertion by the navigation-assisted method. Also, another study disclosed that the duration of distal femoral nail screws insertion by the navigation method was significantly more than the conventional method [14]. However, according to the conclusion of another research, a significant decrease was observed in the duration of screwing for pedicle screw insertion by the navigation method compared to the free-hand method [12]. Additionally, for nail screw insertion, a significant decrease (22%) in the duration of operation and screw insertion was observed in the navigation method compared to the conventional method [9].
The discrepancies between our results and the mentioned results may be caused by the different nature and design of the studies and their various populations.
5. Conclusion
The use of navigation as a new technology in orthopedics may have a significant impact on the process of distal IMN screw insertion. Although the accuracy of both methods was almost the same, the navigation method reduces the frequency and times of radiation exposure for screw placement. Further well-designed studies with greater sample sizes are required to clarify and compare the consequences of the conventional C-arm method and C-arm-based navigation method for distal Kuntcher screw insertion in patients with the femur or tibia fractures.
Study strengths and limitations
The present investigation has several strengths, including comparing consequences of the conventional C-arm method and C-arm-based navigation method for distal Kuntcher screw insertion in fractures of the long bones of the lower limb, for the first time. Also, appropriate sample size and robust statistical analysis can be considered other strengths. However, connecting and stabilizing the reference to the Kuntcher, the placement space of the calibration frame, sterilizing various parts, and communication with radiographic systems are among the most critical limitations of the present study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran University of Medical Sciences.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Mohammad Hosein Nabian; Methodology: Mehdi Komijanii; Data collection, investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all the surgeons, medical staff, and research team members who contributed to this study. The authors also thank their patients for their participation and trust. Special thanks to Tehran University of Medical Sciences for providing support and resources throughout the research process.
References
- Wong Wei Kang N, Tan WPJ, Phua YMC, Min ATG, Naidu K, et al. Intramedullary nail: The past, present and the future - a review exploring where the future may lead us. Orthop Rev (Pavia). 2021; 13(2):25546. [DOI:10.52965/001c.25546] [PMID] [PMCID]
- Chao J, Patel A, Shah A. Intramedullary screw fixation comprehensive technique guide for metacarpal and phalanx fractures: Pearls and pitfalls. Plast Reconstr Surg Glob Open. 2021; 9(10):e3895. [DOI:10.1097/GOX.0000000000003895] [PMID] [PMCID]
- Hegde AS, Mane PP, Shetty CB, Thakkar SA. “Screw First” technique to get past nail-jig mismatch in proximal femoral nailing. Indian J Orthop. 2021; 56(4):699-704. [DOI:10.1007/s43465-021-00552-w] [PMID] [PMCID]
- Wang S, Zhang W, Sun J, Wang Y, Fan J, Yu Y, et al. Detection of common anatomical landmarks and vertical trajectories for freehand pedicle screw placement. Ortho Surg. 2023; 15(6):1541-8. [DOI:10.1111/os.13729] [PMID] [PMCID]
- Bäcker HC, Heyland M, Wu CH, Perka C, Stöckle U, Braun KF. Breakage of intramedullary femoral nailing or femoral plating: How to prevent implant failure. Europ J of Med Res. 2022; 27(1):7. [DOI:10.1186/s40001-021-00630-7] [PMID] [PMCID]
- Pennig D, Brug E. [Insertion of distal screws in interlocking nailing using a new free-hand control device (German)]. Unfallchirurg. 1989; 92(7):331-4. [PMID]
- Resubal JR, Morgan DA. Computer-assisted vs conventional mechanical Jig Technique in hip resurfacing arthroplasty. J Arthroplasty. 2009; 24(3):341-50. [DOI:10.1016/j.arth.2007.12.013] [PMID]
- Hsu WE, Yu CH, Chang CJ, Wu HK, Yu TH, Tseng CS. C-Arm image-based surgical path planning method for distal locking of intramedullary nails. Appl Bionics Biomech. 2018; 2018:4530386. [DOI:10.1155/2018/4530386] [PMID] [PMCID]
- Windolf M, Schroeder J, Fliri L, Dicht B, Liebergall M, Richards RG. Reinforcing the role of the conventional C-arm - a novel method for simplified distal interlocking. BMC Musculoskelet Disord. 2012; 13:8. [DOI:10.1186/1471-2474-13-8] [PMID] [PMCID]
- Hebecker A. C-Arm-Based Navigation. In: Stiehl JB, Konermann WH, Haaker RG, DiGioia AM, editors. Navigation and MIS in orthopedic surgery. Berlin: Springer; 2007. [DOI:10.1007/978-3-540-36691-1_3]
- Euler E, Heining S, Riquarts C, Mutschler W. C-arm-based three-dimensional navigation: A preliminary feasibility study. Comput Aided Surg. 2003; 8(1):35-41. [DOI:10.3109/10929080309146101] [PMID]
- Guo F, Dai J, Zhang J, Ma Y, Zhu G, Shen J, et al. Individualized 3D printing navigation template for pedicle screw fixation in upper cervical spine. Plos One. 2017; 12(2):e0171509. [DOI:10.1371/journal.pone.0171509] [PMID] [PMCID]
- Elmi-Terander A, Burström G, Nachabé R, Fagerlund M, Ståhl F, Charalampidis A, et al. Augmented reality navigation with intraoperative 3D imaging vs fluoroscopy-assisted free-hand surgery for spine fixation surgery: A matched-control study comparing accuracy. Sci Rep. 2020; 10(1):707. [DOI:10.1038/s41598-020-57693-5] [PMID] [PMCID]
- Hawi N, Liodakis E, Suero EM, Stuebig T, Citak M, Krettek C. Radiological outcome and intraoperative evaluation of a computer-navigation system for femoral nailing: A retrospective cohort study. Injury. 2014; 45(10):1632-6. [DOI:10.1016/j.injury.2014.05.039] [PMID]
- Suhm N, Messmer P, Zuna I, Jacob LA, Regazzoni P. Fluoroscopic guidance versus surgical navigation for distal locking of intramedullary implants. A prospective, controlled clinical study. Injury. 2004; 35(6):567-74. [DOI:10.1016/S0020-1383(03)00312-7] [PMID]
Type of Study: Research Article |
Subject:
Trauma
Received: 2022/02/11 | Accepted: 2022/04/18 | Published: 2022/11/1
Received: 2022/02/11 | Accepted: 2022/04/18 | Published: 2022/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
