

Volume 10, Issue 4 (11-2023)
JROS 2023, 10(4): 245-250 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Najd Mazhar F, Hasan A, Sadeghzadeh M, Mahmoudinasab O. Irreducible Radial Head Dislocation in Pediatric Patients With Monteggia Fracture: A Series of Nine Patients. JROS 2023; 10 (4) :245-250
URL: http://jros.iums.ac.ir/article-1-2250-en.html
URL: http://jros.iums.ac.ir/article-1-2250-en.html



1- Department of Orthopedics,Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 1457 kb]
(322 Downloads)
| Abstract (HTML) (1157 Views)

Conclusion
Spontaneous reduction of the radial head in the context of Monteggia fractures may not occur in a subset of pediatric patients, requiring an open reduction to adequately address the cause of irreducibility. The interposed annular ligament is this population’s most frequent cause of irreducibility. Although less frequent, PIN interposition requires more awareness because inappropriate management can result in severe nerve damage.
The present study had some limitations. The main limitation was the small number of patients. Another limitation was the retrospective design, which did not allow functional evaluation of outcomes.
Ethical Considerations
Compliance with ethical guidelines
Written informed consents were obtained from the patients for the publication of these case series and accompanying images.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Farid Najd Mazhar, and Majid Sadegh Zadeh; Methodology, and writing: Omid Mahmoudi Nasab and Ahmad Hasan.
Conflict of interest
The authors declared no conflict of interest.
References
Full-Text: (236 Views)
Introduction
Monteggia fractures are characterized by an ulnar shaft fracture concurrent with radial head dislocation [1]. Radial head spontaneous reduction is expected following the close reduction and internal fixation of the ulnar fracture because the tension on the surrounding soft tissues, including the annular ligament, is relieved [2]. However, spontaneous reduction of the radial head may not occur for various reasons, such as the interposed radial nerve and capsule [3, 4].
Irreducible radial head in the context of Monteggia fracture represents a challenging orthopedic injury [3]. While the diagnosis and management of Monteggia fractures have been extensively studied, irreducible radial head dislocation poses unique clinical and therapeutic dilemmas [3]. Persistent dislocation despite attempted closed reduction maneuvers requires a surgical intervention [3]. However, due to the rare incidence of this condition, the data on this condition are very limited, particularly in the pediatric population with unique anatomical and developmental considerations [5].
This study aims to report the characteristic features and interposed elements in nine pediatric patients with irreducible radial head dislocation in the context of Monteggia fractures.
Methods
The institutional review board approved this case series. The medical profiles of nine pediatric patients with Monteggia fractures who underwent surgery for the treatment of irreducible radial head dislocation in our referral orthopedic hospital between 2007 and 2024 were retrospectively reviewed. Skeletally mature (closed growth plates) patients were excluded from this study.
Management protocol
A senior surgeon managed all the patients. Eight of nine patients presented with primary injuries. In one patient, the radial head was initially reduced in another center, and one week after the index management, the patient was referred to our center with re-dislocation (case 5).
First, we attempted to closely reduce the ulnar fractures under sedation. If closed reduction was not practical, open surgery was selected to reduce and fix the fracture under general anesthesia. Fixation was performed using Kirschner wires, intramedullary nails, or plates, depending on the fracture type. Subsequently, we attempted close radial head reduction. If close reduction of the radial head was unsuccessful, an open reduction was made using a Kocher [6] or extensor digitorum communis splitting approach [6]. These approaches were extended anteriorly to explore the posterior interosseous nerve (PIN) and evaluate its interposition if required. The causes of radial head irreducibility were recorded during surgical repost. After radial head reduction, elbow stability was manually checked over the full range of motion under direct vision, and it proved to be stable in all patients.
Data collection
The collected information included the age and sex, laterality of injury, hand dominancy, mechanism of injury, associated injuries, duration from injury to surgery, type and site of ulnar fracture, procedure performed for managing ulnar fracture, and the direction of radial head dislocation. Our main finding of interest was the cause of radial head irreducibility in this series of pediatric patients.
Results
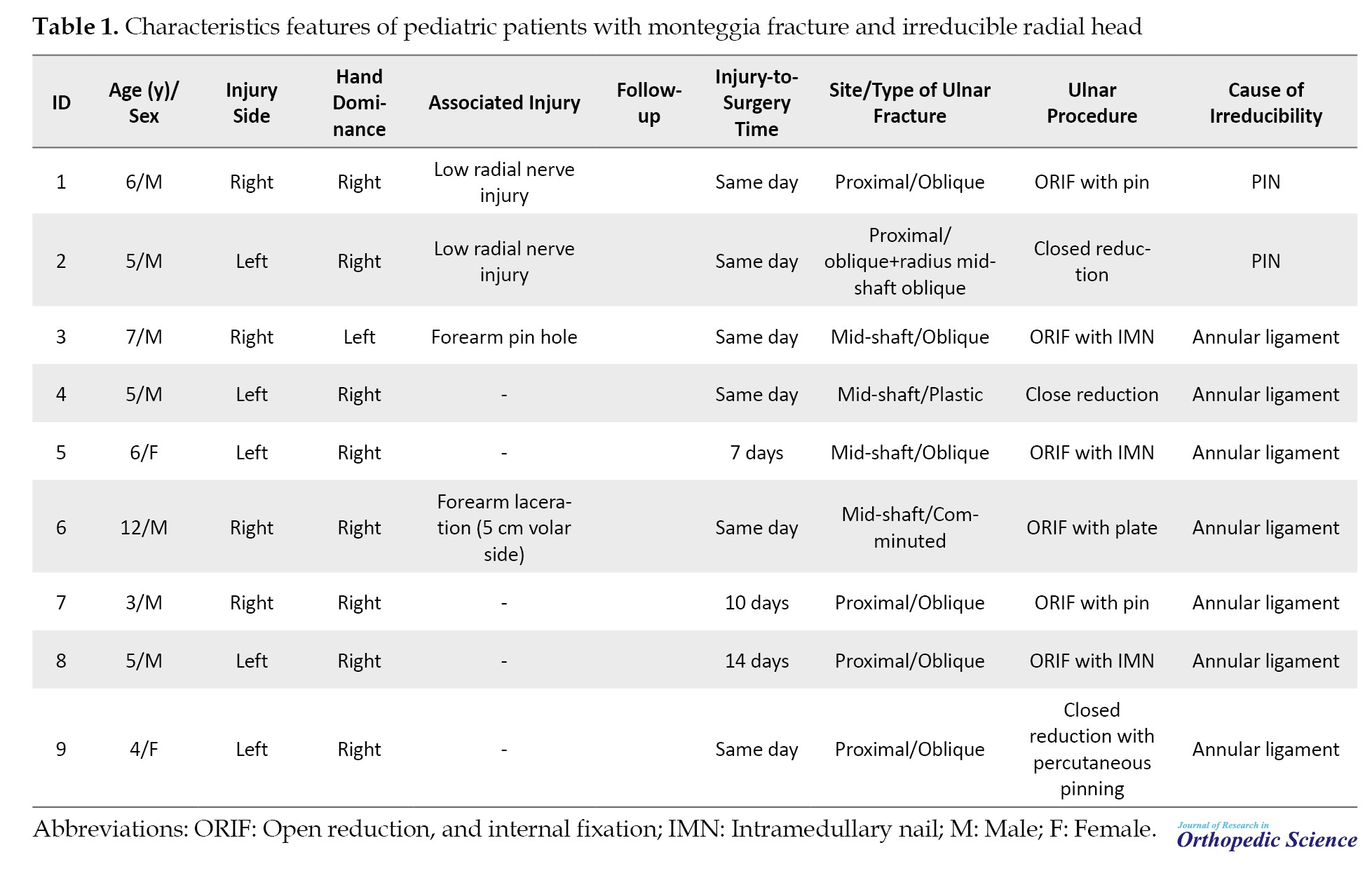
The study population included seven men (77.8%) and two women (22.2%) with a mean age of 5.9±4.1 years (range 3-12). Injury was more frequent in the non-dominant hand (n=6, 66.7%). The mechanism of injury decreased in all patients. Four (44.4%) patients had associated injuries. The most frequent site of ulnar fracture was proximal ulna (n=5, 55.5%). Oblique fractures were the most common ulnar fractures (n=7, 77.8%). Ulnar fractures were managed with open reduction and internal fixation in six patients (66.7%) and close reduction in three (33.7%). In all patients, the radial head was dislocated in the anterior direction. The cause of irreducibility was interposed annular ligament in seven patients (77.8%) (ure 1a) and interposed PIN in two patients (22.2%) (ure 1b). Table 1 presents patient characteristics.
No radial head re-dislocation or subluxation was observed until the last follow-up visit. No complications, such as heterotopic ossification, were observed on the patients’ follow-up radiographs.
Discussion
This study evaluated the interposed element in a series of nine pediatric patients with Monteggia fracture and irreducible radial head. The cause of irreducibility was interposed annular ligament in seven patients and PIN in two patients. The problem was identified in one patient as pseudo-reduction because it was initially reduced in another center and re-dislocated after one week when the patient was referred to our hospital for re-reduction. No re-dislocation or subluxation of the radial head was observed in patients after we resolved interposed elements.
The irreducibility of the radial head in pediatric Monteggia fracture has been reported in several cases [4, 7, 8, 9, 10]. However, owing to the rare incidence of this condition, the number of case series studies in the pediatric population is limited. Abe et al. [11] reported 17 irreducible radial head dislocation cases in pediatric Monteggia lesions. The mean age was 2.7 to 12.1 years. The boy’s involvement occurred twice as soon as the girl’s injury. A similar boy-to-girl ratio was observed in this study. The proximal metaphysis was the most common ulnar fracture site in both studies. In the study by Abe et al. [11], greenstick fracture was the most frequent type of ulnar fracture, while oblique fracture was the least frequent. In the present study, oblique fractures were the most common ulnar fractures. In a study by Abe et al. [11], the radial head was dislocated in various directions. However, it was dislocated anteriorly in all patients in the present study. The problem was identified as pseudo-reduction in 10 patients in the study by Abe et al. and only one patient in the present study. In both studies, annular ligament interposition was the most common cause of radial head irreducibility.
PIN is regarded as the less frequent cause of radial head irreducibility in pediatric patients with Monteggia fractures because it was observed in only one of 17 patients in the study by Abe et al [11]. and two of nine patients in the present study. Aversano et al. reported irreducible radial head in pediatrics with Monteggia fracture, none of which were interposed by PIN [4]. Although PIN interposition is less common in pediatric patients with Monteggia fractures, its management requires more awareness because inappropriate management might result in severe nerve damage. In three patients studied by Abe et al., attempts at close reduction led to PIN interposition between the capitellum and the radial head, and exploration of the radiocapitellar joint after five months showed serious nerve damage, requiring finger extension reconstruction using tendon transfer [11]. Other authors reported the same experience [12, 13]. Therefore, surgical exploration of the involved nerve is required in patients with symptoms of radial nerve injury.
A study by Tan et al. revealed that even if the radiographic evaluation shows a reduction in the radial head, the annular ligaments may be interposed in most pediatric patients with Monteggia fractures. Accordingly, the authors emphasized that radiologic radial head reduction often does not represent anatomic radial head reduction and suggested annular ligament reduction in these patients [14]. They also suggested frequent radiographic examinations because hidden annular ligament interposition can result in pseudo-reduction and re-dislocation of the radial head in forearm pronation [14], as observed in 10 of 17 patients of the study by Abe et al. [11] and one patient of the present study.
Abdelgawad et al. suggested a new technique as an alternative to open reduction for indirect reduction of the radial head by manipulating the ulnar fracture in a subset of Monteggia patients. Their technique proposed that creating a flexion moment at the ulnar might reduce the anteriorly dislocated Bado type I Monteggia fracture-dislocation. They successfully treated two cases of pediatric Monteggia with this method [15]. Although this technique can avoid complications associated with open reduction, more extensive studies are required to better understand this method’s efficacy and long-term outcomes.
Monteggia fractures are characterized by an ulnar shaft fracture concurrent with radial head dislocation [1]. Radial head spontaneous reduction is expected following the close reduction and internal fixation of the ulnar fracture because the tension on the surrounding soft tissues, including the annular ligament, is relieved [2]. However, spontaneous reduction of the radial head may not occur for various reasons, such as the interposed radial nerve and capsule [3, 4].
Irreducible radial head in the context of Monteggia fracture represents a challenging orthopedic injury [3]. While the diagnosis and management of Monteggia fractures have been extensively studied, irreducible radial head dislocation poses unique clinical and therapeutic dilemmas [3]. Persistent dislocation despite attempted closed reduction maneuvers requires a surgical intervention [3]. However, due to the rare incidence of this condition, the data on this condition are very limited, particularly in the pediatric population with unique anatomical and developmental considerations [5].
This study aims to report the characteristic features and interposed elements in nine pediatric patients with irreducible radial head dislocation in the context of Monteggia fractures.
Methods
The institutional review board approved this case series. The medical profiles of nine pediatric patients with Monteggia fractures who underwent surgery for the treatment of irreducible radial head dislocation in our referral orthopedic hospital between 2007 and 2024 were retrospectively reviewed. Skeletally mature (closed growth plates) patients were excluded from this study.
Management protocol
A senior surgeon managed all the patients. Eight of nine patients presented with primary injuries. In one patient, the radial head was initially reduced in another center, and one week after the index management, the patient was referred to our center with re-dislocation (case 5).
First, we attempted to closely reduce the ulnar fractures under sedation. If closed reduction was not practical, open surgery was selected to reduce and fix the fracture under general anesthesia. Fixation was performed using Kirschner wires, intramedullary nails, or plates, depending on the fracture type. Subsequently, we attempted close radial head reduction. If close reduction of the radial head was unsuccessful, an open reduction was made using a Kocher [6] or extensor digitorum communis splitting approach [6]. These approaches were extended anteriorly to explore the posterior interosseous nerve (PIN) and evaluate its interposition if required. The causes of radial head irreducibility were recorded during surgical repost. After radial head reduction, elbow stability was manually checked over the full range of motion under direct vision, and it proved to be stable in all patients.
Data collection
The collected information included the age and sex, laterality of injury, hand dominancy, mechanism of injury, associated injuries, duration from injury to surgery, type and site of ulnar fracture, procedure performed for managing ulnar fracture, and the direction of radial head dislocation. Our main finding of interest was the cause of radial head irreducibility in this series of pediatric patients.
Results
The study population included seven men (77.8%) and two women (22.2%) with a mean age of 5.9±4.1 years (range 3-12). Injury was more frequent in the non-dominant hand (n=6, 66.7%). The mechanism of injury decreased in all patients. Four (44.4%) patients had associated injuries. The most frequent site of ulnar fracture was proximal ulna (n=5, 55.5%). Oblique fractures were the most common ulnar fractures (n=7, 77.8%). Ulnar fractures were managed with open reduction and internal fixation in six patients (66.7%) and close reduction in three (33.7%). In all patients, the radial head was dislocated in the anterior direction. The cause of irreducibility was interposed annular ligament in seven patients (77.8%) (ure 1a) and interposed PIN in two patients (22.2%) (ure 1b). Table 1 presents patient characteristics.
No radial head re-dislocation or subluxation was observed until the last follow-up visit. No complications, such as heterotopic ossification, were observed on the patients’ follow-up radiographs.
Discussion
This study evaluated the interposed element in a series of nine pediatric patients with Monteggia fracture and irreducible radial head. The cause of irreducibility was interposed annular ligament in seven patients and PIN in two patients. The problem was identified in one patient as pseudo-reduction because it was initially reduced in another center and re-dislocated after one week when the patient was referred to our hospital for re-reduction. No re-dislocation or subluxation of the radial head was observed in patients after we resolved interposed elements.
The irreducibility of the radial head in pediatric Monteggia fracture has been reported in several cases [4, 7, 8, 9, 10]. However, owing to the rare incidence of this condition, the number of case series studies in the pediatric population is limited. Abe et al. [11] reported 17 irreducible radial head dislocation cases in pediatric Monteggia lesions. The mean age was 2.7 to 12.1 years. The boy’s involvement occurred twice as soon as the girl’s injury. A similar boy-to-girl ratio was observed in this study. The proximal metaphysis was the most common ulnar fracture site in both studies. In the study by Abe et al. [11], greenstick fracture was the most frequent type of ulnar fracture, while oblique fracture was the least frequent. In the present study, oblique fractures were the most common ulnar fractures. In a study by Abe et al. [11], the radial head was dislocated in various directions. However, it was dislocated anteriorly in all patients in the present study. The problem was identified as pseudo-reduction in 10 patients in the study by Abe et al. and only one patient in the present study. In both studies, annular ligament interposition was the most common cause of radial head irreducibility.
PIN is regarded as the less frequent cause of radial head irreducibility in pediatric patients with Monteggia fractures because it was observed in only one of 17 patients in the study by Abe et al [11]. and two of nine patients in the present study. Aversano et al. reported irreducible radial head in pediatrics with Monteggia fracture, none of which were interposed by PIN [4]. Although PIN interposition is less common in pediatric patients with Monteggia fractures, its management requires more awareness because inappropriate management might result in severe nerve damage. In three patients studied by Abe et al., attempts at close reduction led to PIN interposition between the capitellum and the radial head, and exploration of the radiocapitellar joint after five months showed serious nerve damage, requiring finger extension reconstruction using tendon transfer [11]. Other authors reported the same experience [12, 13]. Therefore, surgical exploration of the involved nerve is required in patients with symptoms of radial nerve injury.
A study by Tan et al. revealed that even if the radiographic evaluation shows a reduction in the radial head, the annular ligaments may be interposed in most pediatric patients with Monteggia fractures. Accordingly, the authors emphasized that radiologic radial head reduction often does not represent anatomic radial head reduction and suggested annular ligament reduction in these patients [14]. They also suggested frequent radiographic examinations because hidden annular ligament interposition can result in pseudo-reduction and re-dislocation of the radial head in forearm pronation [14], as observed in 10 of 17 patients of the study by Abe et al. [11] and one patient of the present study.
Abdelgawad et al. suggested a new technique as an alternative to open reduction for indirect reduction of the radial head by manipulating the ulnar fracture in a subset of Monteggia patients. Their technique proposed that creating a flexion moment at the ulnar might reduce the anteriorly dislocated Bado type I Monteggia fracture-dislocation. They successfully treated two cases of pediatric Monteggia with this method [15]. Although this technique can avoid complications associated with open reduction, more extensive studies are required to better understand this method’s efficacy and long-term outcomes.
Conclusion
Spontaneous reduction of the radial head in the context of Monteggia fractures may not occur in a subset of pediatric patients, requiring an open reduction to adequately address the cause of irreducibility. The interposed annular ligament is this population’s most frequent cause of irreducibility. Although less frequent, PIN interposition requires more awareness because inappropriate management can result in severe nerve damage.
The present study had some limitations. The main limitation was the small number of patients. Another limitation was the retrospective design, which did not allow functional evaluation of outcomes.
Ethical Considerations
Compliance with ethical guidelines
Written informed consents were obtained from the patients for the publication of these case series and accompanying images.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Farid Najd Mazhar, and Majid Sadegh Zadeh; Methodology, and writing: Omid Mahmoudi Nasab and Ahmad Hasan.
Conflict of interest
The authors declared no conflict of interest.
References
- Delpont M, Louahem D, Cottalorda J. Monteggia injuries. Orthop Traumatol Surg Res. 2018; 104(1S):S113-20. [DOI:10.1016/j.otsr.2017.04.014] [PMID]
- Rehim SA, Maynard MA, Sebastin SJ, Chung KC. Monteggia fracture dislocations: A historical review. J Hand Surg Am. 2014; 39(7):1384-94. [DOI:10.1016/j.jhsa.2014.02.024] [PMID] [PMCID]
- Tanner C, Johnson T, Kolahi K, Husak L, Hoekzema N. Irreducible monteggia fracture: Interposed radial nerve and capsule. JSES Open Access. 2017; 1(2):85-89. [DOI:10.1016/j.jses.2017.06.003] [PMID] [PMCID]
- Aversano F, Kepler CK, Blanco JS, Green DW. Rare cause of block to reduction after radial head dislocation in children. J Orthop Trauma. 2011; 25(4):e38-41. [DOI:10.1097/BOT.0b013e3181dc245d] [PMID]
- Sánchez Saba JE, Abrego MO, Bosio ST, Puigdevall M, Maenza R. [Isolated irreducible anterior radial head dislocation in a child: A rare case report (Spanish)]. Arch Argent Pediatr. 2018; 116(4):e630-4. [DOI:10.5546/aap.2018.e630] [PMID]
- Berdusco R, Louati H, Desloges W, Papp SR, Pollock JW. Lateral elbow exposures: The extensor digitorum communis split compared with the kocher approach. JBJS Essent Surg Tech. 2015; 5(4):e30. [DOI:10.2106/JBJS.ST.N.00048] [PMID] [PMCID]
- Ha T, Grant S, Huntley JS. Monteggia type IV fracture in a child with radial head dislocation irreducible by closed means: A case report. BMC Res Notes. 2014; 7:539. [DOI:10.1186/1756-0500-7-539] [PMID] [PMCID]
- Bradley MP, Tashjian RZ, Eberson CP. Irreducible radial head dislocation in a child: A case report. Am J Orthop. 2007; 36(5):E76-9. [PMID]
- Demirel M, Sağlam Y, Tunalı O. Posterior interosseous nerve palsy associated with neglected pediatric monteggia fracture-dislocation: A case report. Int J Surg Case Rep. 2016; 27:102-6. [DOI:10.1016/j.ijscr.2016.08.011] [PMID] [PMCID]
- Takase K, Mizuochi J. Irreducible dislocation of the radial head with undisplaced olecranon fracture in a child: A case report. J Pediatr Orthop B. 2011; 20(5):345-8. [DOI:10.1097/BPB.0b013e32834534cb] [PMID]
- Abe M, Kumano H, Kinoshita A, Hirofuji S. Irreducible dislocation of the radial head associated with pediatric monteggia lesions. J Am Acad Orthop Surg Glob Res Rev. 2018; 2(5):e035. [DOI:10.5435/JAAOSGlobal-D-17-00035] [PMID] [PMCID]
- Li H, Cai QX, Shen PQ, Chen T, Zhang ZM, Zhao L. Posterior interosseous nerve entrapment after Monteggia fracture-dislocation in children. Chin J Traumatol. 2013; 16(3):131-5. [PMID]
- Spar I. A neurologic complication following Monteggia fracture. Clin Orthop Relat Res. 1977(122):207-9. [DOI:10.1097/00003086-197701000-00031]
- Tan JW, Mu MZ, Liao GJ, Li JM. Pathology of the annular ligament in paediatric Monteggia fractures. Injury. 2008; 39(4):451-5. [DOI:10.1016/j.injury.2007.07.010] [PMID]
- Abdelgawad AA, Wey AJ, Khalifa R, Shoulah S, Thabet AM. Irreducible radial head in monteggia fracture dislocation; Is there an alternative to open reduction? Acta Sci Orthop. 2021; 4(7):10-5. [DOI:10.31080/ASOR.2021.04.0327]
Type of Study: Research Article |
Subject:
Hand surgery / Elbow
Received: 2023/07/4 | Accepted: 2023/10/7 | Published: 2023/11/1
Received: 2023/07/4 | Accepted: 2023/10/7 | Published: 2023/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
