

Volume 10, Issue 4 (11-2023)
JROS 2023, 10(4): 217-224 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Chehrassan M, Nikouei F, Shakeri M, Moeini J, Ameri Mahabadi E, Ghandhari H. ACDF Instead of Anterior Cervical Discectomy and Fusion. JROS 2023; 10 (4) :217-224
URL: http://jros.iums.ac.ir/article-1-2252-en.html
URL: http://jros.iums.ac.ir/article-1-2252-en.html
Mohammadreza Chehrassan1 

 , Farshad Nikouei1 , Mohammadreza Shakeri1 , Javad Moeini1 , Ebrahim Ameri Mahabadi1 , Hasan Ghandhari1
, Farshad Nikouei1 , Mohammadreza Shakeri1 , Javad Moeini1 , Ebrahim Ameri Mahabadi1 , Hasan Ghandhari1
, Farshad Nikouei1 , Mohammadreza Shakeri1 , Javad Moeini1 , Ebrahim Ameri Mahabadi1 , Hasan Ghandhari1
1- Bone and Joint Reconstruction Research Center, Shafayahyaeian Hospital, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Cervical disc herniation, Cervical lordosis, Anterior cervical discectomy and fusion (ACDF), Global spine alignment, Pelvic tilt, Fusion level
Full-Text [PDF 4053 kb]
(344 Downloads)
| Abstract (HTML) (1396 Views)

Results
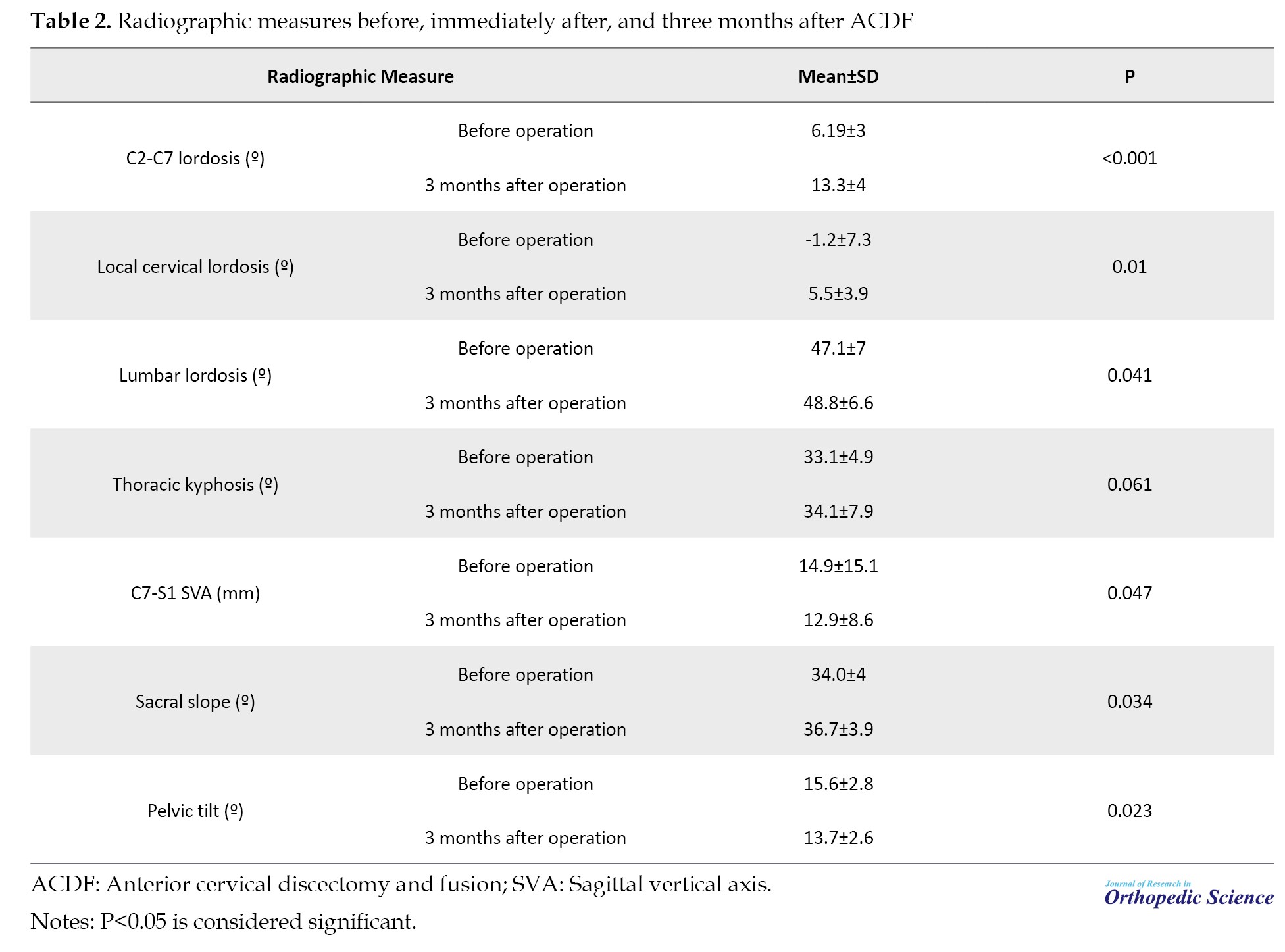
All parameters were altered 3 months postoperatively. While global and local cervical lordosis, thoracic kyphosis, lumbar lordosis, and sacral slope increased, the C7-S1 SVA and pelvic tilt decreased. These results were statistically significant, except for thoracic kyphosis (Table 2).
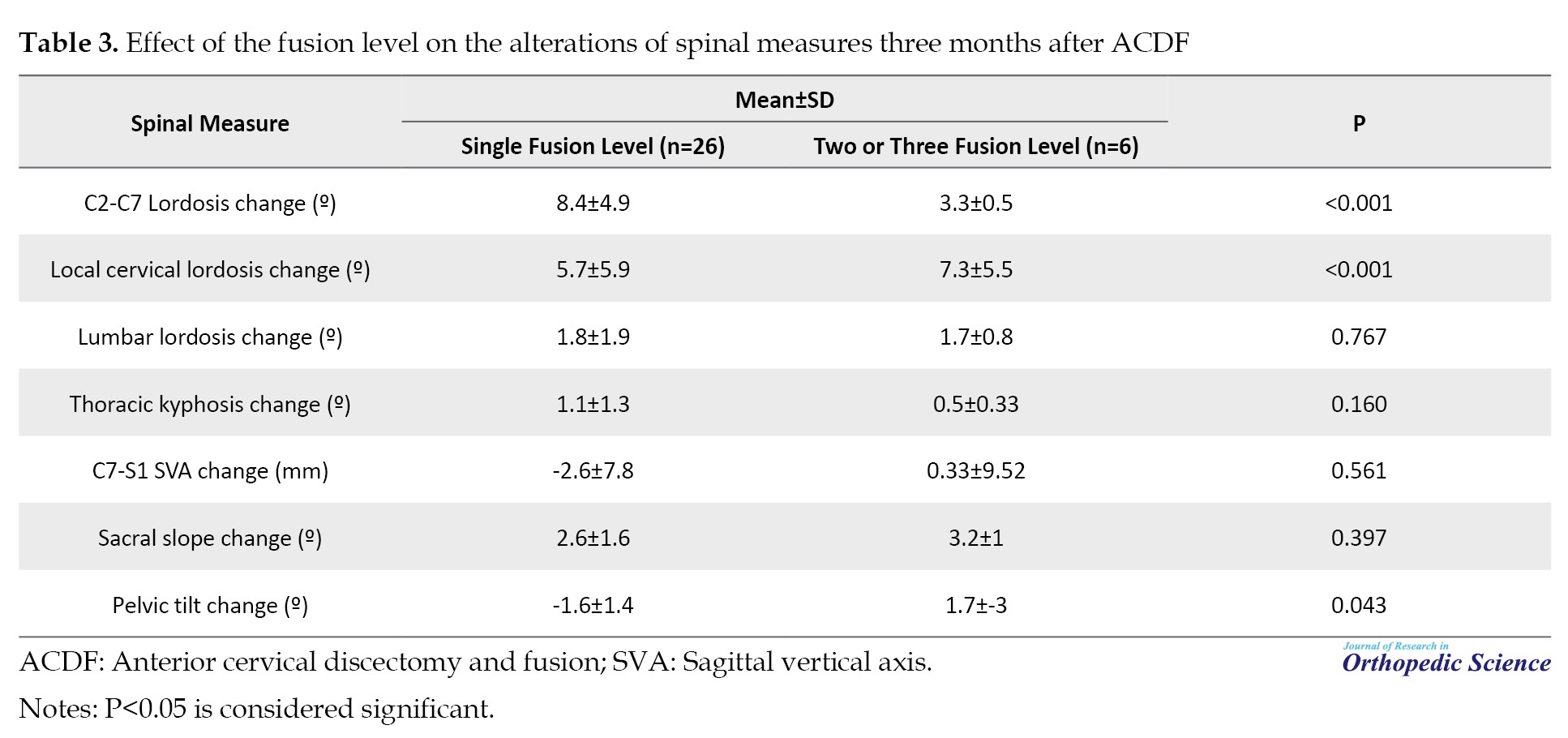
Considering the number of fused levels by ACDF, three months postoperatively, global cervical lordosis, local lordosis, and pelvic tilt were significantly different between patients with one fusion level and those with two or three fusion levels. In this respect, the global cervical lordosis correction was greater in cases with a single fusion level (P<0.001); however, the local cervical lordosis correction was significantly higher in patients with two or three fusion levels (P<0.001). Pelvic tilt change was significantly greater in cases with multiple fusion levels (P=0.043). Other spinal parameter changes, including lumbar lordosis, thoracic kyphosis, C7-S1 SVA, and sacral slope, were not significantly different between one, two, or three fusion levels (Table 3).
Discussion
Reciprocal changes in cervical spine alignment and thoracolumbar alignment have been considered in earlier studies [10-14]. Ha et al. evaluated cervical spine parameters after treating thoracolumbar deformity in 49 patients. Patients were divided into low and high C7 SVA groups. In the lower C7 SVA group, cervical lordosis significantly increased after thoracolumbar deformity correction, while in the high C7 SVA group, cervical lordosis showed a significant reduction after the operation. In multilinear regression analysis, preoperative cervical parameters predicted postoperative cervical lordosis [10]. Yu et al. evaluated the relationship between the cervical spine and the global spine alignment. Cervical spine alignment significantly correlated with global spine alignment in asymptomatic subjects and those with cervical spondylosis. In the cervical spondylotic group, cervical angles were significantly different in patients with different Roussouly types [11].
Changes in spinopelvic parameters after ACDF have also been reported in previous studies. Huang et al. evaluated changes in spinopelvic sagittal alignment in 133 patients with cervical spondylosis who underwent ACDF. They observed several significant changes in global spinal alignment, including thoracic kyphosis, sacral slope, spinal sacral angles, and lumbar lordosis [15]. Kim et al. aimed to determine whole spine sagittal alignment and pelvic alignment changes in 48 patients after ACDF. Twelve months after the operation, the pelvic tilt significantly increased, while the sacral slope significantly reduced. A significant correlation was observed between cervical lordosis and SVA. In addition, the SVA was significantly associated with pelvic tilt and sacral slope. They concluded that ACDF impacts whole spine sagittal alignment, particularly in patients with high cervical lordosis. In these cases, restoration of cervical lordosis caused reciprocal changes in pelvic tilt and sacral slope, mediated by a shortened SVA [5]. Similarly, in the present study, restoration of lumbar lordosis following ACDF led to alterations in other spinal curvatures, including the whole-spine sagittal and pelvic alignment.
Patients who undergo multilevel cervical fusions restore greater amounts of cervical lordosis compared to patients with a single-level fusion [16]. Accordingly, multilevel fusion is expected to have a more significant effect on global spinal alignment. In the present study, segmental lordosis correction was significantly greater in patients with multilevel fusion. In addition, changes in global spinal alignment, specifically pelvic tilt correction, were more frequent in the multilevel fusion group. These observations reveal that cervical fusion levels are associated with post-ACDF alterations in global spinal alignment.
Altogether, the results of the current study confirmed the reciprocal correlation between cervical alignment and global spinal alignment in patients who underwent ACDF. Moreover, the present study reveals that while the number of fused levels affects local and global cervical lordosis, this entity has no role in global spine alignment and spino-pelvic parameters except for pelvic tilt. Future studies may use this information for personalized correction of global spine alignment during the ACDF procedure.
Conclusion
Alterations in cervical alignment affect global spinal alignment in patients with cervical disc herniation who undergo ACDF. While ACDF and local and global cervical restoration affect global spine alignment and spinopelvic parameters, the number of fusion levels does not affect these entities, except for pelvic tilt.
The present study has some limitations. The primary limitation was the small number of patients, which did not allow multivariate data analysis. Another limitation was the short follow-up period. Therefore, future studies with larger patient numbers and longer follow-up periods can help further understand the relationship between the cervical and global alignment of the spine and factors affecting the association among patients undergoing ACDF.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1402.305). All procedures performed in this study involving human participants were by the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards. No information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript could be used to identify patients.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Mohammadreza Chehrassan; Investigation: Hasan Ghandhari; Data collection and analysis: Javad Moeini; Supervision: Ebrahim Amerimahabadi; Writing: Farshad Nikoei, and Mohammadreza Shakeri.
Conflict of interest
The authors declared no conflict of interest.
References
Full-Text: (281 Views)
Introduction
Cervical lordosis is a vital physiological curvature of the human spine. Normal cervical curvature is necessary for maintaining balance and various human activities, such as motor functions, mastication, breathing, vocal production, and eye movement. It also acts as a shock-absorbing mechanism in ambulatory functions [1, 2]. In a bilateral connection, malalignment in the cervical curvature also has a detrimental effect on the alignment of the spine in other parts, including thoracolumbar angle and pelvic alignment [3-5].
Along with the increasingly sedentary lifestyle in recent years, a higher incidence of abnormal cervical curvature is reported in the literature [6, 7]. Cervical disc herniation is one of the leading causes of abnormal cervical curvature [8]. Anterior cervical discectomy and fusion (ACDF) combines spinal decompression and fusion surgery to treat herniated cervical discs and correct cervical lordosis [9].
Considering the direct relationship between cervical and global spine alignment, correction of cervical lordosis improves whole-spine and pelvic sagittal alignment [3-5]. However, due to the small number of studies, the impact of ACDF on global spinal alignment is not clearly understood. This study was conducted to evaluate spinal alignment changes following correction of cervical lordosis in a series of patients with cervical disc herniation who underwent ACDF.
Methods
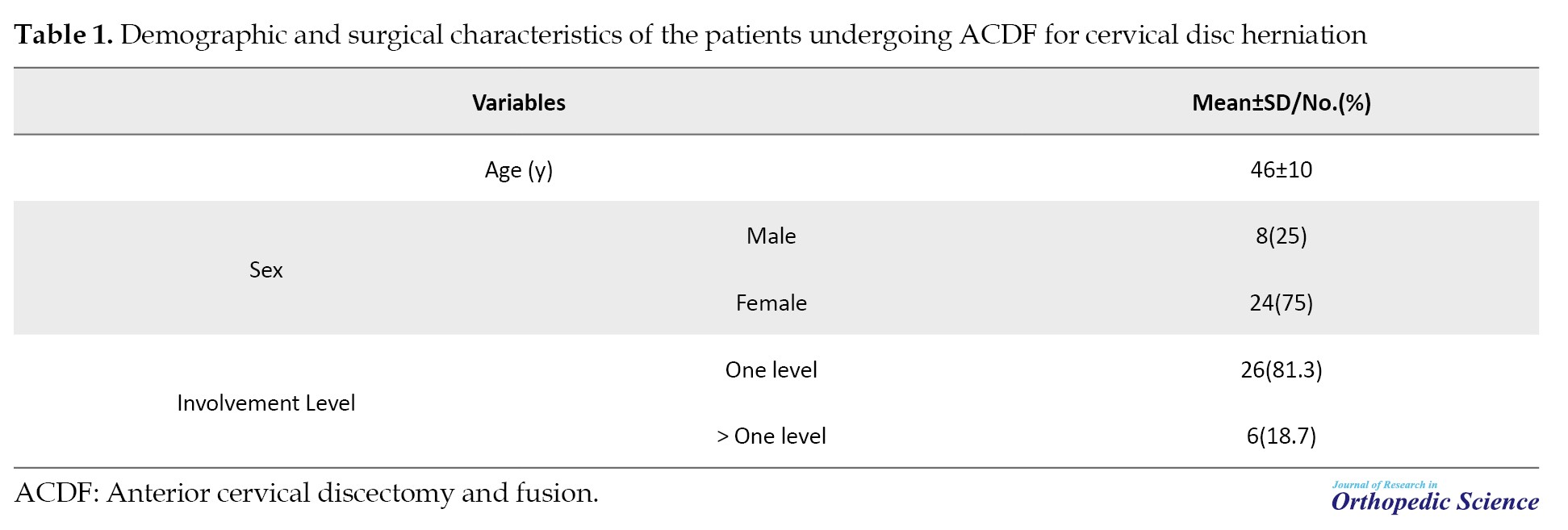
The medical profiles of patients who underwent ACDF at our hospital between January 2017 and December 2022 were retrospectively reviewed. The inclusion criteria included patients with degenerative cervical disc herniation who underwent ACDF if they underwent preoperative and postoperative EOS® imaging. The exclusion criteria included patients with other medical conditions, such as trauma, tumor, or infection, as well as those with a history of previous spine surgery or tandem spinal stenosis. Finally, 32 patients who met the study criteria were included. Table 1 presents the patient demographics and surgical features.
Radiographic assessments
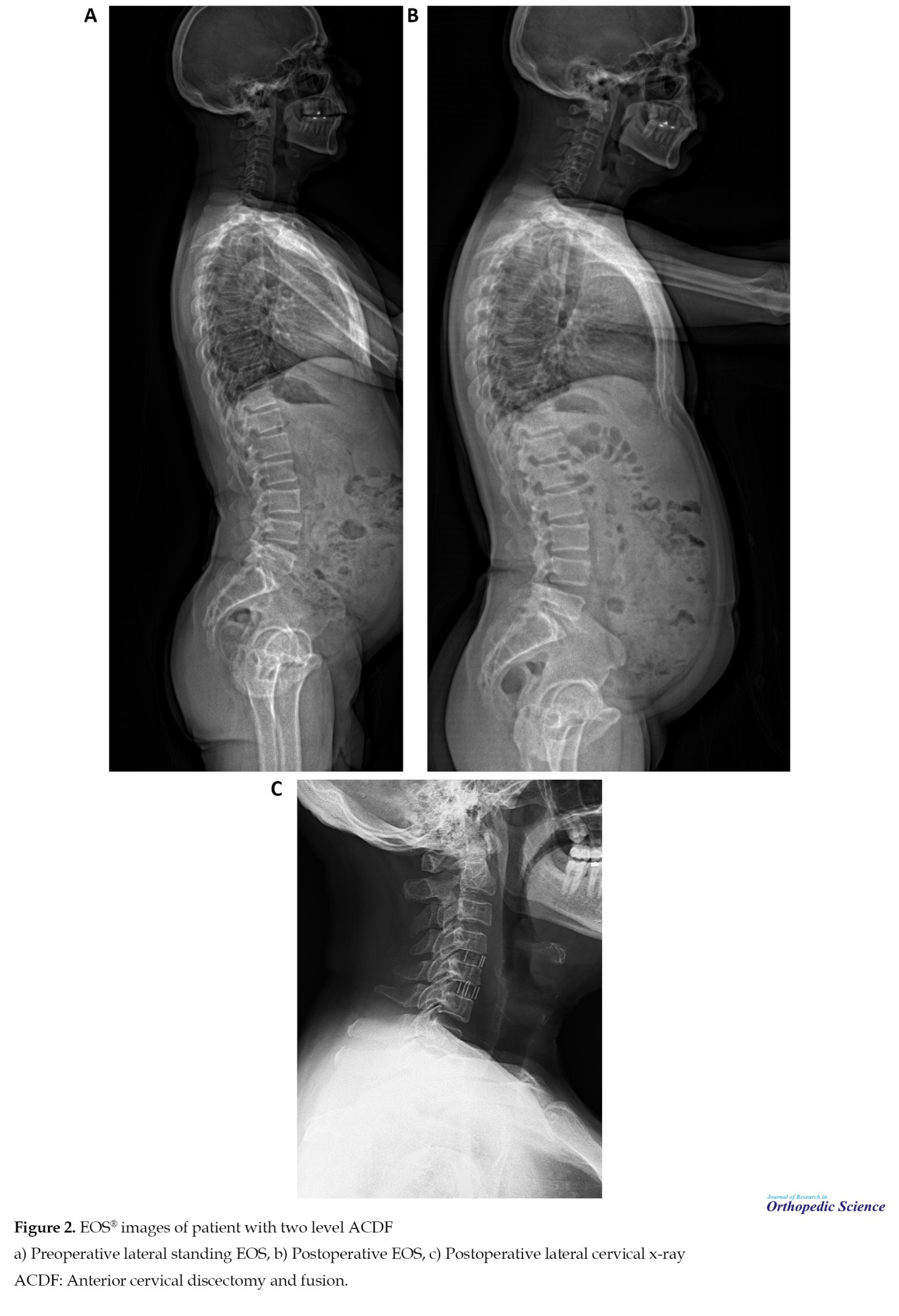
Radiographic evaluations were conducted on whole-spine EOS® images obtained preoperatively and three months postoperatively. The assessments included measurement of cervical local lordosis at the level of ACDF, global cervical lordosis, thoracic kyphosis, lumbar lordosis, and whole-spine alignment by measuring the C7-S1 sagittal vertical axis (SVA) and spino-pelvic parameters. Global cervical lordosis was assessed by calculating the Cobb angle between distal endplates C2 and C7. Local cervical lordosis was measured as lordosis of the involved cervical vertebrae in patients who underwent ACDF. Spino-pelvic variables were evaluated by measuring the pelvic tilt and sacral slope (Figures 1 and 2).
Cervical lordosis is a vital physiological curvature of the human spine. Normal cervical curvature is necessary for maintaining balance and various human activities, such as motor functions, mastication, breathing, vocal production, and eye movement. It also acts as a shock-absorbing mechanism in ambulatory functions [1, 2]. In a bilateral connection, malalignment in the cervical curvature also has a detrimental effect on the alignment of the spine in other parts, including thoracolumbar angle and pelvic alignment [3-5].
Along with the increasingly sedentary lifestyle in recent years, a higher incidence of abnormal cervical curvature is reported in the literature [6, 7]. Cervical disc herniation is one of the leading causes of abnormal cervical curvature [8]. Anterior cervical discectomy and fusion (ACDF) combines spinal decompression and fusion surgery to treat herniated cervical discs and correct cervical lordosis [9].
Considering the direct relationship between cervical and global spine alignment, correction of cervical lordosis improves whole-spine and pelvic sagittal alignment [3-5]. However, due to the small number of studies, the impact of ACDF on global spinal alignment is not clearly understood. This study was conducted to evaluate spinal alignment changes following correction of cervical lordosis in a series of patients with cervical disc herniation who underwent ACDF.
Methods
The medical profiles of patients who underwent ACDF at our hospital between January 2017 and December 2022 were retrospectively reviewed. The inclusion criteria included patients with degenerative cervical disc herniation who underwent ACDF if they underwent preoperative and postoperative EOS® imaging. The exclusion criteria included patients with other medical conditions, such as trauma, tumor, or infection, as well as those with a history of previous spine surgery or tandem spinal stenosis. Finally, 32 patients who met the study criteria were included. Table 1 presents the patient demographics and surgical features.
Radiographic assessments
Radiographic evaluations were conducted on whole-spine EOS® images obtained preoperatively and three months postoperatively. The assessments included measurement of cervical local lordosis at the level of ACDF, global cervical lordosis, thoracic kyphosis, lumbar lordosis, and whole-spine alignment by measuring the C7-S1 sagittal vertical axis (SVA) and spino-pelvic parameters. Global cervical lordosis was assessed by calculating the Cobb angle between distal endplates C2 and C7. Local cervical lordosis was measured as lordosis of the involved cervical vertebrae in patients who underwent ACDF. Spino-pelvic variables were evaluated by measuring the pelvic tilt and sacral slope (Figures 1 and 2).
Results
All parameters were altered 3 months postoperatively. While global and local cervical lordosis, thoracic kyphosis, lumbar lordosis, and sacral slope increased, the C7-S1 SVA and pelvic tilt decreased. These results were statistically significant, except for thoracic kyphosis (Table 2).
Considering the number of fused levels by ACDF, three months postoperatively, global cervical lordosis, local lordosis, and pelvic tilt were significantly different between patients with one fusion level and those with two or three fusion levels. In this respect, the global cervical lordosis correction was greater in cases with a single fusion level (P<0.001); however, the local cervical lordosis correction was significantly higher in patients with two or three fusion levels (P<0.001). Pelvic tilt change was significantly greater in cases with multiple fusion levels (P=0.043). Other spinal parameter changes, including lumbar lordosis, thoracic kyphosis, C7-S1 SVA, and sacral slope, were not significantly different between one, two, or three fusion levels (Table 3).
Discussion
Reciprocal changes in cervical spine alignment and thoracolumbar alignment have been considered in earlier studies [10-14]. Ha et al. evaluated cervical spine parameters after treating thoracolumbar deformity in 49 patients. Patients were divided into low and high C7 SVA groups. In the lower C7 SVA group, cervical lordosis significantly increased after thoracolumbar deformity correction, while in the high C7 SVA group, cervical lordosis showed a significant reduction after the operation. In multilinear regression analysis, preoperative cervical parameters predicted postoperative cervical lordosis [10]. Yu et al. evaluated the relationship between the cervical spine and the global spine alignment. Cervical spine alignment significantly correlated with global spine alignment in asymptomatic subjects and those with cervical spondylosis. In the cervical spondylotic group, cervical angles were significantly different in patients with different Roussouly types [11].
Changes in spinopelvic parameters after ACDF have also been reported in previous studies. Huang et al. evaluated changes in spinopelvic sagittal alignment in 133 patients with cervical spondylosis who underwent ACDF. They observed several significant changes in global spinal alignment, including thoracic kyphosis, sacral slope, spinal sacral angles, and lumbar lordosis [15]. Kim et al. aimed to determine whole spine sagittal alignment and pelvic alignment changes in 48 patients after ACDF. Twelve months after the operation, the pelvic tilt significantly increased, while the sacral slope significantly reduced. A significant correlation was observed between cervical lordosis and SVA. In addition, the SVA was significantly associated with pelvic tilt and sacral slope. They concluded that ACDF impacts whole spine sagittal alignment, particularly in patients with high cervical lordosis. In these cases, restoration of cervical lordosis caused reciprocal changes in pelvic tilt and sacral slope, mediated by a shortened SVA [5]. Similarly, in the present study, restoration of lumbar lordosis following ACDF led to alterations in other spinal curvatures, including the whole-spine sagittal and pelvic alignment.
Patients who undergo multilevel cervical fusions restore greater amounts of cervical lordosis compared to patients with a single-level fusion [16]. Accordingly, multilevel fusion is expected to have a more significant effect on global spinal alignment. In the present study, segmental lordosis correction was significantly greater in patients with multilevel fusion. In addition, changes in global spinal alignment, specifically pelvic tilt correction, were more frequent in the multilevel fusion group. These observations reveal that cervical fusion levels are associated with post-ACDF alterations in global spinal alignment.
Altogether, the results of the current study confirmed the reciprocal correlation between cervical alignment and global spinal alignment in patients who underwent ACDF. Moreover, the present study reveals that while the number of fused levels affects local and global cervical lordosis, this entity has no role in global spine alignment and spino-pelvic parameters except for pelvic tilt. Future studies may use this information for personalized correction of global spine alignment during the ACDF procedure.
Conclusion
Alterations in cervical alignment affect global spinal alignment in patients with cervical disc herniation who undergo ACDF. While ACDF and local and global cervical restoration affect global spine alignment and spinopelvic parameters, the number of fusion levels does not affect these entities, except for pelvic tilt.
The present study has some limitations. The primary limitation was the small number of patients, which did not allow multivariate data analysis. Another limitation was the short follow-up period. Therefore, future studies with larger patient numbers and longer follow-up periods can help further understand the relationship between the cervical and global alignment of the spine and factors affecting the association among patients undergoing ACDF.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1402.305). All procedures performed in this study involving human participants were by the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards. No information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript could be used to identify patients.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Mohammadreza Chehrassan; Investigation: Hasan Ghandhari; Data collection and analysis: Javad Moeini; Supervision: Ebrahim Amerimahabadi; Writing: Farshad Nikoei, and Mohammadreza Shakeri.
Conflict of interest
The authors declared no conflict of interest.
References
- Been E, Shefi S, Soudack M. Cervical lordosis: The effect of age and gender. Spine J. 2017; 17(6):880-8. [DOI:10.1016/j.spinee.2017.02.007] [PMID]
- Norton TC, Oakley PA, Harrison DE. Re-establishing the cervical lordosis after whiplash: A chiropractic biophysics® spinal corrective care methods pre-auto injury and post-auto injury case report with follow-up. J Phys Ther Sci. 2023; 35(3):270-5. [DOI:10.1589/jpts.35.270] [PMID] [PMCID]
- Smith JS, Shaffrey CI, Lafage V, Blondel B, Schwab F, Hostin R, et al. Spontaneous improvement of cervical alignment after correction of global sagittal balance following pedicle subtraction osteotomy. J Neurosurg Spine. 2012; 17(4):300-7. [DOI:10.3171/2012.6.SPINE1250] [PMID]
- Lee SH, Son ES, Seo EM, Suk KS, Kim KT. Factors determining cervical spine sagittal balance in asymptomatic adults: correlation with spinopelvic balance and thoracic inlet alignment. Spine J. 2015; 15(4):705-12. [DOI:10.1016/j.spinee.2013.06.059] [PMID]
- Kim JH, Park JY, Yi S, Kim KH, Kuh SU, Chin DK, et al. Anterior cervical discectomy and fusion alters whole-spine sagittal alignment. Yonsei Med J. 2015; 56(4):1060-70. [DOI:10.3349/ymj.2015.56.4.1060] [PMID] [PMCID]
- Han SM, Wen JX, Cao L, Wu HZ, Liu C, Yang C, et al. Sagittal morphology of the cervical spine in adolescent idiopathic scoliosis: A retrospective case-control study. Quant Imaging Med Surg. 2022; 12(6):3049-60. [DOI:10.21037/qims-21-902] [PMID] [PMCID]
- Shin Y, Han K, Lee YH. Temporal trends in cervical spine curvature of south korean adults assessed by deep learning system segmentation, 2006-2018. JAMA Netw Open. 2020; 3(10):e2020961. [DOI:10.1001/jamanetworkopen.2020.20961] [PMID] [PMCID]
- Gao K, Zhang J, Lai J, Liu W, Lyu H, Wu Y, et al. Correlation between cervical lordosis and cervical disc herniation in young patients with neck pain. Medicine. 2019; 98(31):e16545. [DOI:10.1097/MD.0000000000016545] [PMID] [PMCID]
- Rhee JM, Ju KL. Anterior cervical discectomy and fusion. JBJS Essent Surg Tech. 2016; 6(4):e37. [DOI:10.2106/JBJS.ST.15.00056] [PMID] [PMCID]
- Ha Y, Schwab F, Lafage V, Mundis G, Shaffrey C, Smith J, et al. Reciprocal changes in cervical spine alignment after corrective thoracolumbar deformity surgery. Eur Spine J. 2014; 23(3):552-9. [DOI:10.1007/s00586-013-2953-8] [PMID] [PMCID]
- Yu M, Zhao WK, Li M, Wang SB, Sun Y, Jiang L, et al. Analysis of cervical and global spine alignment under Roussouly sagittal classification in Chinese cervical spondylotic patients and asymptomatic subjects. Eur Spine J. 2015; 24(6):1265-73. [DOI:10.1007/s00586-015-3832-2] [PMID]
- Yoshida G, Alzakri A, Pointillart V, Boissiere L, Obeid I, Matsuyama Y, et al. Global spinal alignment in patients with cervical spondylotic myelopathy. Spine. 2018; 43(3):E154-62. [DOI:10.1097/BRS.0000000000002253] [PMID]
- Patel PD, Arutyunyan G, Plusch K, Vaccaro A Jr, Vaccaro AR. A review of cervical spine alignment in the normal and degenerative spine. J Spine Surg. 2020; 6(1):106-23. [DOI:10.21037/jss.2020.01.10] [PMID] [PMCID]
- Mizutani J, Strom R, Abumi K, Endo K, Ishii K, Yagi M, et al. How cervical reconstruction surgery affects global spinal alignment. Neurosurgery. 2019; 84(4):898-907. [DOI:10.1093/neuros/nyy141] [PMID] [PMCID]
- Huang DN, Yu M, Xu NF, Li M, Wang SB, Sun Y,et al. The relationship between changes of cervical sagittal alignment after anterior cervical discectomy and fusion and spino-pelvic sagittal alignment under roussouly classification: A four-year follow-up study. BMC Musculoskelet Disord. 2017; 18(1):87. [DOI:10.1186/s12891-017-1447-y] [PMID] [PMCID]
- Basques BA, Louie PK, Mormol J, Khan JM, Movassaghi K, Paul JC, et al. Multi-versus single-level anterior cervical discectomy and fusion: Comparing sagittal alignment, early adjacent segment degeneration, and clinical outcomes. Eur Spine J. 2018; 27(11):2745-53. [DOI:10.1007/s00586-018-5677-y] [PMID]
Type of Study: Research Article |
Subject:
Spine surgery
Received: 2023/08/3 | Accepted: 2023/10/9 | Published: 2023/11/1
Received: 2023/08/3 | Accepted: 2023/10/9 | Published: 2023/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
