

Volume 11, Issue 2 (May 2024)
JROS 2024, 11(2): 97-106 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yeganeh A, Haghighi M, Kazemi S, Amani H, Zareie B. Investigating the Prevalence of Depression in Older People With Hip Fractures. JROS 2024; 11 (2) :97-106
URL: http://jros.iums.ac.ir/article-1-2276-en.html
URL: http://jros.iums.ac.ir/article-1-2276-en.html



1- Department of Orthopaedic Surgery, Trauma and Injury Research Center, School of Medicine, Rasoul Akram Hospital, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Psychiatry, School of Medicine, Urmia University of Medical Sciences, Urmia, Iran.
3- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. & Department of Orthopedics, Imam Khomeini Hospital, Urmia University of Medical Sciences, Urmia, Iran.
4- Department of Orthopedics, Imam Khomeini Hospital, Urmia University of Medical Sciences, Urmia, Iran.
5- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Psychiatry, School of Medicine, Urmia University of Medical Sciences, Urmia, Iran.
3- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. & Department of Orthopedics, Imam Khomeini Hospital, Urmia University of Medical Sciences, Urmia, Iran.
4- Department of Orthopedics, Imam Khomeini Hospital, Urmia University of Medical Sciences, Urmia, Iran.
5- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Hip fractures, Depression in older people, Trochanteric fractures, Peri-hip fractures, Mental health assessment after the fracture
Full-Text [PDF 540 kb]
(335 Downloads)
| Abstract (HTML) (796 Views)
Full-Text: (241 Views)
Introduction
The most frequent psychiatric disorder is depression all over the world and a leading cause of disability [1]. The prevalence of depression is 13.7% in the Iranian population [2]. Depression significantly impacts quality of life and imposes a substantial economic burden [3, 4].
Hip fracture is a serious medical condition that disrupts general health [5] and is among the most common physical damages in older people [6]. Surgical repair of hip fractures is one of the most frequently performed orthopedic procedures, particularly in older adults compared to younger populations. This injury predominantly affects patients over 60 years of age, who often have multiple comorbidities [7]. Globally, 120 million individuals suffer from hip fractures [8], and approximately 25000 older adults experience hip fractures in the United States every year [9].
Old age, osteoarthritis, malnutrition, muscle weakness, visual impairment, and osteoporosis are the primary risk factors for hip fractures. However, osteoporosis is the most critical factor [9]. In addition to osteoporosis, several other medical conditions, such as hypertension, diabetes mellitus, and cerebrovascular diseases, contribute to prolonged recovery and increased mortality rates [10]. The incidence of hip fractures is estimated to be approximately 1.5 million cases annually and is projected to rise to around 2.6 million cases per year by 2025 [11]. Furthermore, mortality associated with hip fractures is significant, with post-fracture mortality increasing 4.6-fold in men and 2.8-fold in women within one year of the fracture [12]. Given the increasing global aging population, hip fractures are expected to become a major public health concern among older people.
Accidental falls among older adults typically occur at home, resulting in hip fractures with or without pre-existing comorbidities. This condition marks the beginning of a series of healthcare challenges, involving numerous healthcare professionals (such as surgeons, physicians, and physiotherapists), family members, social workers, and caregivers. Today, hip fractures have emerged as a significant global healthcare issue, presenting unique challenges and substantial economic implications for patients, their families, and healthcare budgets [13]. The financial burden of managing such patients is remarkably high. According to a 2013 national report, the average cost per patient was estimated at 64000 pound in the United Kingdom and 8 billion USD in the United States, directly correlating with variables such as hospital stay duration, surgical timing, and the availability of specialized orthopedic-geriatric units [14]. Numerous studies on hip fractures have focused not only on the socioeconomic aspects of patient management but also on the high mortality rates associated with this condition [15].
Experiencing a hip fracture can be a sudden and life-altering event, significantly increasing patient vulnerability over time. Hip fractures pose a significant threat to all aspects of functional status, particularly in older people. Loss of independence, physical limitations, pain, and fatigue are major complications of hip fractures, making recovery particularly challenging for older adults [16]. Additionally, hip fractures are associated with high mortality rates [17]. The acute mortality rate is approximately 5%, while one-year post-fracture mortality ranges between 15% and 25%. It is estimated that 20% of patients with hip fractures never regain their ability to walk independently [8], and fewer than 30% return to their previous activity levels [5]. Early post-fracture mortality remains high, with rates of 8%-10% within the first 30 days and approximately 20%-28% within the first year. However, only one-third of these deaths are directly attributed to the fracture itself [17-20].
Cognitive impairment is another factor contributing to reduced functional recovery during the healing process [21]. Depression is the most prevalent mood and cognitive disorder among older adults and is recognized as one of the primary complications following hip fractures in this population [22]. Depression is frequently observed during hip fracture recovery and is considered a leading cause of disability in affected patients. A key clinical aspect of depression in hip fracture patients is the interplay between emotional status and functional recovery. Several studies have confirmed the negative impact of depression on functional outcomes and mortality [22, 23]. In patients with hip fracture, depression is associated with an increased risk of infection, reduced survival rates, and poorer prognosis [5]. Additionally, 15% of older individuals report clinical symptoms of depression. Depression is linked to increased disability, poor physical performance, falls, and low bone density, all of which elevate the risk of osteoporotic fractures. Older adults taking antidepressants or sedatives may also be at higher risk of falls and fractures. Moreover, patients with depression exhibit poorer recovery following fractures [24].
As no previous studies have examined this issue in Iran, the present study aims to investigate the prevalence of depression in elderly patients with trochanteric or hip fractures.
Methods
This cross-sectional study was conducted through a complete enumeration of patients over the age of 65 with trochanteric or hip fractures region who were admitted and treated in the Orthopedic Department of Imam Khomeini Hospital in 2021 (Urmia, Iran). In the study title, we used the term hip fractures region to broadly refer to various fractures in this area, including subtrochanteric and femoral head fractures. However, our analysis specifically focused on femoral neck and intertrochanteric fractures, as these are more prevalent in the elderly population we examined. A questionnaire was used to collect demographic data, including age, gender, disease duration, place of residence, and history of psychiatric medication use. After explaining the study objectives and obtaining informed consent, each patient was given the geriatric depression scale (GDS) to assess depressive symptoms. Patients were followed up three months post-fracture, during which they completed the GDS again. Changes in depression scores between the acute phase (during the fracture) and three months after the fracture were analyzed. Data collection tools included a demographic questionnaire and the GDS [25].
Data analysis
Data were analyzed using SPSS software, version 16. Quantitative variables were presented as Mean±SD, while categorical variables were reported as percentages. The paired t-test was used to compare depression scores at the time of fracture and three months post-fracture to assess changes over time.
Results
The Mean±SD age of patients with trochanteric or periprosthetic hip fractures over 65 years old at Imam Khomeini Hospital is 74.9±8.9 years. The mean depression score (at the time of fracture) for these patients was 4.27±2.98. The paired samples t-test reveals no significant difference in depression levels between the onset of the fracture and three months later (P>0.05) (Table 1).

There is also no significant difference in depression levels based on gender (P>0.05). Women show a greater increase in depression three months after the fracture compared to men, but this is not statistically significant. For age groups, there is no significant difference in depression levels between patients aged 65 to 75 and those over 85 years old (P>0.05). However, a significant difference is noted for the 75 to 85 age group (P<0.05). At the onset, depression levels were 3.9, 4.6, and 5.2 for the respective age groups, indicating higher depression with increasing age. The paired samples t-test reveals no significant difference in depression levels based on place of residence (P>0.05). Depression levels at the onset for undiagnosed, under 5 years, 5 to 10 years, and 10 to 20 years were 4, 6.8, 7.6, and 9.5, respectively, suggesting higher depression with longer diagnosis duration. There is also no significant difference in depression levels based on income (P>0.05) (Table 2).
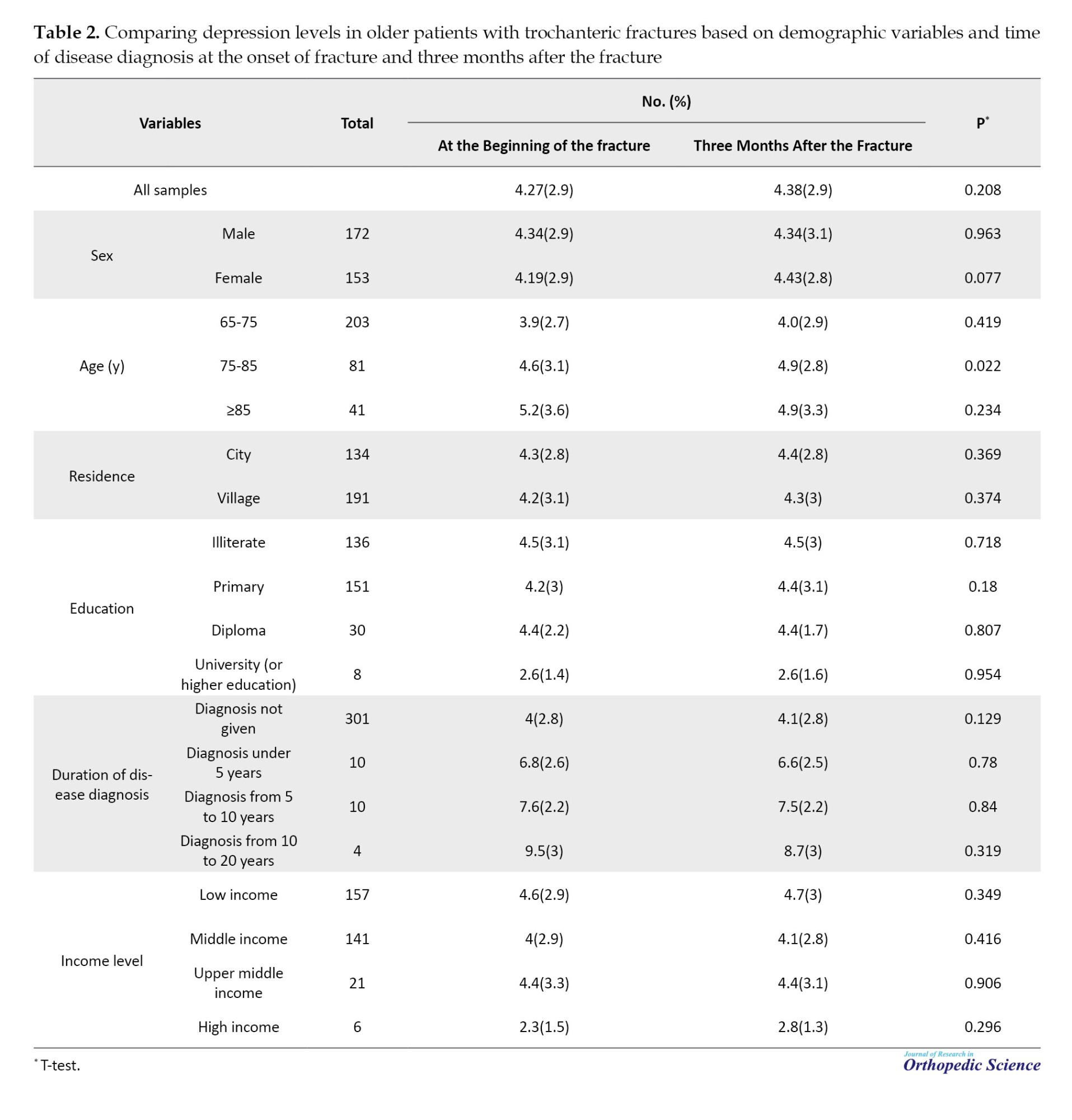
At the onset, depression levels for low, average, good, and excellent income were 4.6, 4, 4.4, and 3.2, respectively, indicating lower depression in higher income patients. Lastly, the paired samples t-test reveals no significant difference in depression levels based on education (P>0.05). The analysis of the distribution of gender indicates that 50.9% of patients with femoral neck fractures, 52.5% of patients with intertrochanteric fractures, and 69.6% of patients with both femoral neck and intertrochanteric fractures are male (Table 3).

Discussion
Aging is widely recognized as a significant risk factor for fractures. Research has demonstrated a clear correlation between advancing age and the incidence of hip fractures. As the population ages, both the frequency of hip fractures and the associated treatment costs are increasing. In the study by Cheng et al. [9], significant statistical differences were observed in the incidence of hip fractures among different age groups. However, as the population ages, the loss of bone and muscle mass increases the risk of falls, which can lead to fractures [26].
Aging also plays an important role in the occurrence of depression. Studies indicate that both the prevalence and incidence of major depression approximately double between the ages of 70 and 85 [27]. Given that age is a recognized risk factor for both hip fractures and depression, it is plausible that advancing age may contribute to an increased risk of developing depression after experiencing a hip fracture.
In our study, no significant difference was observed in depression rates at the onset of fracture and three months post-fracture among age groups 65–75 and over 85 years (P>0.05). However, in the 75–85 age group, a significant difference was found between depression rates at the time of fracture and three months post-fracture (P=0.022). The depression rates in the 65–75, 75–85, and over 85 age groups were 3.9%, 4.6%, and 5.2%, respectively, indicating that depression rates increased with age.
The prevalence of depression is affected by its baseline occurrence within the population and the duration of symptoms. Research shows that depressive symptoms tend to rise during the final years of life [28]. In older age groups, the prevalence of depressive disorders in both men and women has been reported to surpass 85%. Prior research has emphasized the importance of accurately diagnosing depression in the elderly [29]. Additionally, findings suggest that one in ten adults experiences severe depressive symptoms, with a higher percentage of older adults being affected [29]. Meta-analyses of prospective studies on depression risk factors in elderly populations have identified four major risk factors: Sleep disorders, disability, previous depression, and female gender [30]. Therefore, a substantial portion of depression among older people may be attributed to these risk factors [24]. Given that these risk factors are common in older individuals, their modification could have a significant impact on public health [31].
In our study, depression was diagnosed in 24 patients before the fracture. The mean duration of diagnosed depression was 7.2±4.6 years. The mean depression score at the onset of fracture was 4.27±2.98. Studies have shown that female gender and event severity are associated with depression [32]. Furthermore, elevated depressive symptoms have been demonstrated to affect functional independence in the early stages of hip fracture care [33]. Postoperative depression diagnosis in hip fracture patients influences their functional outcomes and survival [34].
Hip fracture is a significant and disabling condition in older adults, particularly women. Epidemiological data vary across countries, but globally, hip fractures are estimated to affect 18% of women and 6% of men. A fundamental reason is that functional outcomes reported among survivors differ between genders, with men often exhibiting equivalent or even better functional outcomes than women, despite experiencing higher postoperative complications [35].
In the present study, no significant difference in depression rates three months post-fracture was found between men (P=0.936) and women (P=0.077). However, depression rates increased more in women than in men three months post-fracture, although the difference was not statistically significant. In the study by Shyu et al. [36], the authors found that female patients with lower pre-fracture daily living activity levels were at a higher risk of developing depression.
Among the various factors influencing the epidemiology of hip fractures, gender appears to be the most significant. According to epidemiological data on depression in older people, depression affects women twice as often as men [27]. Several studies have investigated mechanisms linking pain and depression, suggesting that pain can restructure neural pathways to trigger negative depressive symptoms [37-39]. Voshaar et al. identified postoperative pain and baseline anxiety as the strongest independent risk factors for depression [40]. Bruggemann et al. demonstrated that post-injury beliefs and hopelessness influence depression and anxiety levels in patients with hip fractures during the acute injury phase [41]. Long-term risk factors such as loss of ambulation ability and reduced self-care capacity may contribute to the progression of depression.
Studies have also found significant differences in depression prevalence between homebound and semi-homebound elderly individuals [42]. Psychological changes during recovery are also important [43]. Extended sleep duration, reduced activity levels, and severe impacts on daily activities all contribute to feelings of helplessness. Consequently, every stage of psychological and physical change post-surgery can affect the development of depression.
Our study found no significant difference in depression rates at the onset of fracture and three months post-fracture based on patients’ educational levels. At the time of fracture, depression rates among illiterate, primary school, high school, and university-educated patients were 4.5%, 4.2%, 4.4%, and 2.6%, respectively. In the study by Liu et al. [44], researchers distinguished groups of postoperative depressive symptom trajectories. They found that the likelihood of illiteracy was lower among those in the low-risk group compared to those in the high-risk group (P=0.02). Emotional support from family, friends, and the community plays a crucial role in an individual’s psychological well-being, particularly for those with a compromised health-related quality of life [45].
In the present study, no significant difference in depression rates at the onset of fracture and three months post-fracture was observed based on patients’ place of residence or income levels. At the time of fracture, depression rates in patients with poor, moderate, good, and excellent income levels were 4.6%, 4%, 4.4%, and 2.3%, respectively. The findings suggest that depressive symptoms were less severe in patients with higher income levels compared to those with lower income levels. Research has indicated that low socioeconomic status, rural residency, being single, and housing conditions contribute to depressive disorders. However, no direct empirical data have demonstrated a link between post-hip fracture depression and these factors [46].
In the present study, no significant difference in depression rates at the onset of fracture and three months post-fracture was observed based on the duration of depression diagnosis (P>0.05). At the onset of fracture, depression rates in undiagnosed patients, those diagnosed for less than 5 years, those diagnosed for 5–10 years, and those diagnosed for 10–20 years were 4%, 6.8%, 7.6%, and 9.5%, respectively, indicating that longer depression duration was associated with higher depression rates.
Regarding medication management, concerns arise as antidepressants may increase fracture risk and reduce physical function. Agarwal et al. [47] compared physical function in women who were current users versus non-users of antidepressants and found that grip strength in non-users was 13.3% lower than in current users (P=0.04). Wu et al. [48] demonstrated that depression and antidepressant use were independently associated with an increased risk of fractures. Consequently, antidepressant treatment may elevate the risk of secondary fractures in patients experiencing post-hip fracture depression.
Selective serotonin reuptake inhibitors (SSRIs) have been linked to reduced bone mineral density and increased osteoporosis-related fracture risk. Tricyclic antidepressants may elevate fracture risk through mechanisms independent of bone density effects. However, data on the effects of other antidepressants on bone remain insufficient [49]. Elderly patients, who are particularly vulnerable to osteoporosis, may be better suited for non-SSRI antidepressants. Therefore, determining the necessity and appropriate choice of antidepressant therapy for post-hip fracture depression remains unclear. At a minimum, patients with post-hip fracture depression should undergo bone mineral density testing before initiating antidepressant treatment.
Conclusion
The results of this study indicate that the level of depression three months post-fracture was higher in women compared to men, though this difference was not statistically significant. Furthermore, a significant difference was observed in depression levels between the acute phase of the fracture and three months post-fracture in the age group between 75 and 85 years (P=0.022). Specifically, as the age of the patients increased, the severity of depression also increased. Understanding the impact of post-hip fracture depression on patients can assist healthcare providers in developing more comprehensive treatment strategies. Given the high prevalence of depressive disorders in patients with physical illnesses, clinicians need to be familiar with the symptoms, complications, and treatments of depression, as well as the effects of various medications in inducing or exacerbating depressive symptoms. This goal can be achieved through collaborative efforts between different healthcare professionals, including consultations with psychiatrists. Psychiatric counseling should be arranged during hospitalization to facilitate diagnosis, recommend psychosocial interventions, and manage medications. Patients who exhibit high-risk factors should receive appropriate interventions before surgery, rather than after the onset of post-operative depression symptoms, at which point it may be too late. Timely intervention can prevent increased treatment costs and ensure the effectiveness of therapeutic outcomes.
Ethical Considerations
Compliance with ethical guidelines
The study was conducted following the ethical principles outlined in the Helsinki Declaration and was approved by the Ethics Committee of Urmia University of Medical Sciences, Urmia, Iran (Code: IR.UMSU.REC.1400.074). Written informed consent was obtained from all patients before their participation.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Siamak Kazemi; Methodology and literature search strategy: MahMonir Haghighi and Hamed Amani; Investigation and data collection: Ali Yeganeh, Bushra Zareie, and Hamed Amani; Writing the original draft: Ali Yeganeh and Bushra Zareie; Review and editing: Siamak Kazemi and MahMonir Haghighi; Visualization: Bushra Zareie.
Conflict of interest
The authors declared no conflict of interest.
References
The most frequent psychiatric disorder is depression all over the world and a leading cause of disability [1]. The prevalence of depression is 13.7% in the Iranian population [2]. Depression significantly impacts quality of life and imposes a substantial economic burden [3, 4].
Hip fracture is a serious medical condition that disrupts general health [5] and is among the most common physical damages in older people [6]. Surgical repair of hip fractures is one of the most frequently performed orthopedic procedures, particularly in older adults compared to younger populations. This injury predominantly affects patients over 60 years of age, who often have multiple comorbidities [7]. Globally, 120 million individuals suffer from hip fractures [8], and approximately 25000 older adults experience hip fractures in the United States every year [9].
Old age, osteoarthritis, malnutrition, muscle weakness, visual impairment, and osteoporosis are the primary risk factors for hip fractures. However, osteoporosis is the most critical factor [9]. In addition to osteoporosis, several other medical conditions, such as hypertension, diabetes mellitus, and cerebrovascular diseases, contribute to prolonged recovery and increased mortality rates [10]. The incidence of hip fractures is estimated to be approximately 1.5 million cases annually and is projected to rise to around 2.6 million cases per year by 2025 [11]. Furthermore, mortality associated with hip fractures is significant, with post-fracture mortality increasing 4.6-fold in men and 2.8-fold in women within one year of the fracture [12]. Given the increasing global aging population, hip fractures are expected to become a major public health concern among older people.
Accidental falls among older adults typically occur at home, resulting in hip fractures with or without pre-existing comorbidities. This condition marks the beginning of a series of healthcare challenges, involving numerous healthcare professionals (such as surgeons, physicians, and physiotherapists), family members, social workers, and caregivers. Today, hip fractures have emerged as a significant global healthcare issue, presenting unique challenges and substantial economic implications for patients, their families, and healthcare budgets [13]. The financial burden of managing such patients is remarkably high. According to a 2013 national report, the average cost per patient was estimated at 64000 pound in the United Kingdom and 8 billion USD in the United States, directly correlating with variables such as hospital stay duration, surgical timing, and the availability of specialized orthopedic-geriatric units [14]. Numerous studies on hip fractures have focused not only on the socioeconomic aspects of patient management but also on the high mortality rates associated with this condition [15].
Experiencing a hip fracture can be a sudden and life-altering event, significantly increasing patient vulnerability over time. Hip fractures pose a significant threat to all aspects of functional status, particularly in older people. Loss of independence, physical limitations, pain, and fatigue are major complications of hip fractures, making recovery particularly challenging for older adults [16]. Additionally, hip fractures are associated with high mortality rates [17]. The acute mortality rate is approximately 5%, while one-year post-fracture mortality ranges between 15% and 25%. It is estimated that 20% of patients with hip fractures never regain their ability to walk independently [8], and fewer than 30% return to their previous activity levels [5]. Early post-fracture mortality remains high, with rates of 8%-10% within the first 30 days and approximately 20%-28% within the first year. However, only one-third of these deaths are directly attributed to the fracture itself [17-20].
Cognitive impairment is another factor contributing to reduced functional recovery during the healing process [21]. Depression is the most prevalent mood and cognitive disorder among older adults and is recognized as one of the primary complications following hip fractures in this population [22]. Depression is frequently observed during hip fracture recovery and is considered a leading cause of disability in affected patients. A key clinical aspect of depression in hip fracture patients is the interplay between emotional status and functional recovery. Several studies have confirmed the negative impact of depression on functional outcomes and mortality [22, 23]. In patients with hip fracture, depression is associated with an increased risk of infection, reduced survival rates, and poorer prognosis [5]. Additionally, 15% of older individuals report clinical symptoms of depression. Depression is linked to increased disability, poor physical performance, falls, and low bone density, all of which elevate the risk of osteoporotic fractures. Older adults taking antidepressants or sedatives may also be at higher risk of falls and fractures. Moreover, patients with depression exhibit poorer recovery following fractures [24].
As no previous studies have examined this issue in Iran, the present study aims to investigate the prevalence of depression in elderly patients with trochanteric or hip fractures.
Methods
This cross-sectional study was conducted through a complete enumeration of patients over the age of 65 with trochanteric or hip fractures region who were admitted and treated in the Orthopedic Department of Imam Khomeini Hospital in 2021 (Urmia, Iran). In the study title, we used the term hip fractures region to broadly refer to various fractures in this area, including subtrochanteric and femoral head fractures. However, our analysis specifically focused on femoral neck and intertrochanteric fractures, as these are more prevalent in the elderly population we examined. A questionnaire was used to collect demographic data, including age, gender, disease duration, place of residence, and history of psychiatric medication use. After explaining the study objectives and obtaining informed consent, each patient was given the geriatric depression scale (GDS) to assess depressive symptoms. Patients were followed up three months post-fracture, during which they completed the GDS again. Changes in depression scores between the acute phase (during the fracture) and three months after the fracture were analyzed. Data collection tools included a demographic questionnaire and the GDS [25].
Data analysis
Data were analyzed using SPSS software, version 16. Quantitative variables were presented as Mean±SD, while categorical variables were reported as percentages. The paired t-test was used to compare depression scores at the time of fracture and three months post-fracture to assess changes over time.
Results
The Mean±SD age of patients with trochanteric or periprosthetic hip fractures over 65 years old at Imam Khomeini Hospital is 74.9±8.9 years. The mean depression score (at the time of fracture) for these patients was 4.27±2.98. The paired samples t-test reveals no significant difference in depression levels between the onset of the fracture and three months later (P>0.05) (Table 1).
There is also no significant difference in depression levels based on gender (P>0.05). Women show a greater increase in depression three months after the fracture compared to men, but this is not statistically significant. For age groups, there is no significant difference in depression levels between patients aged 65 to 75 and those over 85 years old (P>0.05). However, a significant difference is noted for the 75 to 85 age group (P<0.05). At the onset, depression levels were 3.9, 4.6, and 5.2 for the respective age groups, indicating higher depression with increasing age. The paired samples t-test reveals no significant difference in depression levels based on place of residence (P>0.05). Depression levels at the onset for undiagnosed, under 5 years, 5 to 10 years, and 10 to 20 years were 4, 6.8, 7.6, and 9.5, respectively, suggesting higher depression with longer diagnosis duration. There is also no significant difference in depression levels based on income (P>0.05) (Table 2).
At the onset, depression levels for low, average, good, and excellent income were 4.6, 4, 4.4, and 3.2, respectively, indicating lower depression in higher income patients. Lastly, the paired samples t-test reveals no significant difference in depression levels based on education (P>0.05). The analysis of the distribution of gender indicates that 50.9% of patients with femoral neck fractures, 52.5% of patients with intertrochanteric fractures, and 69.6% of patients with both femoral neck and intertrochanteric fractures are male (Table 3).
Discussion
Aging is widely recognized as a significant risk factor for fractures. Research has demonstrated a clear correlation between advancing age and the incidence of hip fractures. As the population ages, both the frequency of hip fractures and the associated treatment costs are increasing. In the study by Cheng et al. [9], significant statistical differences were observed in the incidence of hip fractures among different age groups. However, as the population ages, the loss of bone and muscle mass increases the risk of falls, which can lead to fractures [26].
Aging also plays an important role in the occurrence of depression. Studies indicate that both the prevalence and incidence of major depression approximately double between the ages of 70 and 85 [27]. Given that age is a recognized risk factor for both hip fractures and depression, it is plausible that advancing age may contribute to an increased risk of developing depression after experiencing a hip fracture.
In our study, no significant difference was observed in depression rates at the onset of fracture and three months post-fracture among age groups 65–75 and over 85 years (P>0.05). However, in the 75–85 age group, a significant difference was found between depression rates at the time of fracture and three months post-fracture (P=0.022). The depression rates in the 65–75, 75–85, and over 85 age groups were 3.9%, 4.6%, and 5.2%, respectively, indicating that depression rates increased with age.
The prevalence of depression is affected by its baseline occurrence within the population and the duration of symptoms. Research shows that depressive symptoms tend to rise during the final years of life [28]. In older age groups, the prevalence of depressive disorders in both men and women has been reported to surpass 85%. Prior research has emphasized the importance of accurately diagnosing depression in the elderly [29]. Additionally, findings suggest that one in ten adults experiences severe depressive symptoms, with a higher percentage of older adults being affected [29]. Meta-analyses of prospective studies on depression risk factors in elderly populations have identified four major risk factors: Sleep disorders, disability, previous depression, and female gender [30]. Therefore, a substantial portion of depression among older people may be attributed to these risk factors [24]. Given that these risk factors are common in older individuals, their modification could have a significant impact on public health [31].
In our study, depression was diagnosed in 24 patients before the fracture. The mean duration of diagnosed depression was 7.2±4.6 years. The mean depression score at the onset of fracture was 4.27±2.98. Studies have shown that female gender and event severity are associated with depression [32]. Furthermore, elevated depressive symptoms have been demonstrated to affect functional independence in the early stages of hip fracture care [33]. Postoperative depression diagnosis in hip fracture patients influences their functional outcomes and survival [34].
Hip fracture is a significant and disabling condition in older adults, particularly women. Epidemiological data vary across countries, but globally, hip fractures are estimated to affect 18% of women and 6% of men. A fundamental reason is that functional outcomes reported among survivors differ between genders, with men often exhibiting equivalent or even better functional outcomes than women, despite experiencing higher postoperative complications [35].
In the present study, no significant difference in depression rates three months post-fracture was found between men (P=0.936) and women (P=0.077). However, depression rates increased more in women than in men three months post-fracture, although the difference was not statistically significant. In the study by Shyu et al. [36], the authors found that female patients with lower pre-fracture daily living activity levels were at a higher risk of developing depression.
Among the various factors influencing the epidemiology of hip fractures, gender appears to be the most significant. According to epidemiological data on depression in older people, depression affects women twice as often as men [27]. Several studies have investigated mechanisms linking pain and depression, suggesting that pain can restructure neural pathways to trigger negative depressive symptoms [37-39]. Voshaar et al. identified postoperative pain and baseline anxiety as the strongest independent risk factors for depression [40]. Bruggemann et al. demonstrated that post-injury beliefs and hopelessness influence depression and anxiety levels in patients with hip fractures during the acute injury phase [41]. Long-term risk factors such as loss of ambulation ability and reduced self-care capacity may contribute to the progression of depression.
Studies have also found significant differences in depression prevalence between homebound and semi-homebound elderly individuals [42]. Psychological changes during recovery are also important [43]. Extended sleep duration, reduced activity levels, and severe impacts on daily activities all contribute to feelings of helplessness. Consequently, every stage of psychological and physical change post-surgery can affect the development of depression.
Our study found no significant difference in depression rates at the onset of fracture and three months post-fracture based on patients’ educational levels. At the time of fracture, depression rates among illiterate, primary school, high school, and university-educated patients were 4.5%, 4.2%, 4.4%, and 2.6%, respectively. In the study by Liu et al. [44], researchers distinguished groups of postoperative depressive symptom trajectories. They found that the likelihood of illiteracy was lower among those in the low-risk group compared to those in the high-risk group (P=0.02). Emotional support from family, friends, and the community plays a crucial role in an individual’s psychological well-being, particularly for those with a compromised health-related quality of life [45].
In the present study, no significant difference in depression rates at the onset of fracture and three months post-fracture was observed based on patients’ place of residence or income levels. At the time of fracture, depression rates in patients with poor, moderate, good, and excellent income levels were 4.6%, 4%, 4.4%, and 2.3%, respectively. The findings suggest that depressive symptoms were less severe in patients with higher income levels compared to those with lower income levels. Research has indicated that low socioeconomic status, rural residency, being single, and housing conditions contribute to depressive disorders. However, no direct empirical data have demonstrated a link between post-hip fracture depression and these factors [46].
In the present study, no significant difference in depression rates at the onset of fracture and three months post-fracture was observed based on the duration of depression diagnosis (P>0.05). At the onset of fracture, depression rates in undiagnosed patients, those diagnosed for less than 5 years, those diagnosed for 5–10 years, and those diagnosed for 10–20 years were 4%, 6.8%, 7.6%, and 9.5%, respectively, indicating that longer depression duration was associated with higher depression rates.
Regarding medication management, concerns arise as antidepressants may increase fracture risk and reduce physical function. Agarwal et al. [47] compared physical function in women who were current users versus non-users of antidepressants and found that grip strength in non-users was 13.3% lower than in current users (P=0.04). Wu et al. [48] demonstrated that depression and antidepressant use were independently associated with an increased risk of fractures. Consequently, antidepressant treatment may elevate the risk of secondary fractures in patients experiencing post-hip fracture depression.
Selective serotonin reuptake inhibitors (SSRIs) have been linked to reduced bone mineral density and increased osteoporosis-related fracture risk. Tricyclic antidepressants may elevate fracture risk through mechanisms independent of bone density effects. However, data on the effects of other antidepressants on bone remain insufficient [49]. Elderly patients, who are particularly vulnerable to osteoporosis, may be better suited for non-SSRI antidepressants. Therefore, determining the necessity and appropriate choice of antidepressant therapy for post-hip fracture depression remains unclear. At a minimum, patients with post-hip fracture depression should undergo bone mineral density testing before initiating antidepressant treatment.
Conclusion
The results of this study indicate that the level of depression three months post-fracture was higher in women compared to men, though this difference was not statistically significant. Furthermore, a significant difference was observed in depression levels between the acute phase of the fracture and three months post-fracture in the age group between 75 and 85 years (P=0.022). Specifically, as the age of the patients increased, the severity of depression also increased. Understanding the impact of post-hip fracture depression on patients can assist healthcare providers in developing more comprehensive treatment strategies. Given the high prevalence of depressive disorders in patients with physical illnesses, clinicians need to be familiar with the symptoms, complications, and treatments of depression, as well as the effects of various medications in inducing or exacerbating depressive symptoms. This goal can be achieved through collaborative efforts between different healthcare professionals, including consultations with psychiatrists. Psychiatric counseling should be arranged during hospitalization to facilitate diagnosis, recommend psychosocial interventions, and manage medications. Patients who exhibit high-risk factors should receive appropriate interventions before surgery, rather than after the onset of post-operative depression symptoms, at which point it may be too late. Timely intervention can prevent increased treatment costs and ensure the effectiveness of therapeutic outcomes.
Ethical Considerations
Compliance with ethical guidelines
The study was conducted following the ethical principles outlined in the Helsinki Declaration and was approved by the Ethics Committee of Urmia University of Medical Sciences, Urmia, Iran (Code: IR.UMSU.REC.1400.074). Written informed consent was obtained from all patients before their participation.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Siamak Kazemi; Methodology and literature search strategy: MahMonir Haghighi and Hamed Amani; Investigation and data collection: Ali Yeganeh, Bushra Zareie, and Hamed Amani; Writing the original draft: Ali Yeganeh and Bushra Zareie; Review and editing: Siamak Kazemi and MahMonir Haghighi; Visualization: Bushra Zareie.
Conflict of interest
The authors declared no conflict of interest.
References
- Brostow DP, Petrik ML, Starosta AJ, Waldo SW. Depression in patients with peripheral arterial disease: A systematic review. Eur J Cardiovasc Nurs. 2017; 16(3):181-93.[DOI:10.1177/1474515116687222] [PMID]
- Nasiri M, Hosseini H, Sakhaei Y, Tabrizi N, Yazdani Cherati J, Abedini M. [Prevalence of psychiatric disorders in patients with multiple sclerosis in Mazandaran, Iran (Persian)]. J Mazandaran Univ Medical Sci. 2016; 26(140):60-70. [Link]
- Schlosser RJ, Gage SE, Kohli P, Soler ZM. Burden of illness: A systematic review of depression in chronic rhinosinusitis. Am J Rhinol Allergy. 2016; 30(4):250-6. [DOI:10.2500/ajra.2016.30.4343] [PMID]
- Battle C, James K, Temblett P. Depression following critical illness: Analysis of incidence and risk factors. J Intensive Care Soc. 2015; 16(2):105-8. [DOI:10.1177/1751143714559904] [PMID]
- Duggal NA, Beswetherick A, Upton J, Hampson P, Phillips AC, Lord JM. Depressive symptoms in hip fracture patients are associated with reduced monocyte superoxide production. Exp Gerontol. 2014; 54:27-34. [DOI:10.1016/j.exger.2014.01.028] [PMID]
- Duggal NA, Upton J, Phillips AC, Hampson P, Lord JM. NK cell immunesenescence is increased by psychological but not physical stress in older adults associated with raised cortisol and reduced perforin expression. Age (Dordr). 2015; 37(1):9748. [DOI:10.1007/s11357-015-9748-2] [PMID]
- Gialanella B, Prometti P, Monguzzi V, Ferlucci C, Baiardi P, Comini L. Determinants of functional outcome in hip fracture: The role of comorbidity. Aging Clin Exp Res. 2018; 30(6):643-50. [DOI:10.1007/s40520-017-0812-x] [PMID]
- Ritchie CS, Kelley AS, Stijacic Cenzer I, Smith AK, Wallhagen ML, Covinsky KE. High Levels of Geriatric Palliative Care Needs in Hip Fracture Patients Before the Hip Fracture. J Pain Symptom Manage. 2016; 52(4):533-8. [DOI:10.1016/j.jpainsymman.2016.07.003] [PMID]
- Cheng BH, Chen PC, Yang YH, Lee CP, Huang KE, Chen VC. Effects of depression and antidepressant medications on hip fracture: A population-based cohort study in Taiwan. Medicine (Baltimore). 2016; 95(36):e4655. [DOI:10.1097/MD.0000000000004655]
- Omsland TK, Emaus N, Tell GS, Magnus JH, Ahmed LA, Holvik K, et al. Mortality following the first hip fracture in Norwegian women and men (1999-2008). A NOREPOS study. Bone. 2014; 63:81-6. [DOI:10.1016/j.bone.2014.02.016] [PMID]
- Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: A systematic epidemiological review. Osteoporos Int. 2009; 20(10):1633-50. [DOI:10.1007/s00198-009-0920-3]
- Lee YK, Kim JW, Lee MH, Moon KH, Koo KH. Trend in the Age-Adjusted Incidence of Hip Fractures in South Korea: Systematic review. Clin Orthop Surg. 2017; 9(4):420-3. [DOI:10.4055/cios.2017.9.4.420] [PMID]
- Marques A, Lourenço Ó, da Silva JA; Portuguese Working Group for the Study of the Burden of Hip Fractures in Portugal. The burden of osteoporotic hip fractures in Portugal: Costs, health related quality of life and mortality. Osteoporos Int. 2015; 26(11):2623-30. [DOI:10.1007/s00198-015-3171-5] [PMID]
- Alexiou KI, Roushias A, Varitimidis SE, Malizos KN. Quality of life and psychological consequences in elderly patients after a hip fracture: A review. Clin Interv Aging. 2018; 13:143-50. [DOI:10.2147/CIA.S150067]
- Huang YF, Liang J, Shyu YL. Number of comorbidities negatively influence psychological outcomes of the elderly following hip fracture in Taiwan. J Aging Health. 2016; 28(8):1343-61. [DOI:10.1177/0898264315618922] [PMID]
- Proctor R, Wade R, Woodward Y, Pendleton N, Baldwin R, Tarrier N, et al. The impact of psychological factors in recovery following surgery for hip fracture. Disabil Rehabil. 2008; 30(9):716-22. [DOI:10.1080/09638280701403536] [PMID]
- Keene GS, Parker MJ, Pryor GA. Mortality and morbidity after hip fractures. BMJ. 1993; 307(6914):1248-50.[DOI:10.1136/bmj.307.6914.1248] [PMID]
- Vestergaard P, Rejnmark L, Mosekilde L. Increased mortality in patients with a hip fracture-effect of pre-morbid conditions and post-fracture complications. Osteoporos Int. 2007; 18(12):1583-93. [DOI:10.1007/s00198-007-0403-3]
- Valizadeh M, Mazloomzadeh S, Golmohammadi S, Larijani B. Mortality after low trauma hip fracture: A prospective cohort study. BMC Musculoskelet Disord. 2012; 13:143. [DOI:10.1186/1471-2474-13-143] [PMID]
- Leibson CL, Tosteson AN, Gabriel SE, Ransom JE, Melton LJ. Mortality, disability, and nursing home use for persons with and without hip fracture: A population-based study. J Am Geriatr Soc. 2002; 50(10):1644-50. [DOI:10.1046/j.1532-5415.2002.50455.x] [PMID]
- Shibasaki K, Asahi T, Mizobuchi K, Akishita M, Ogawa S. Rehabilitation strategy for hip fracture, focused on behavioral psychological symptoms of dementia for older people with cognitive impairment: A nationwide Japan rehabilitation database. Plos One. 2018; 13(7):e0200143. [DOI:10.1371/journal.pone.0200143] [PMID]
- Dubljanin Raspopović E, Marić N, Nedeljković U, Ilić N, Tomanović Vujadinović S, Bumbaširević M. Do depressive symptoms on hospital admission impact early functional outcome in elderly patients with hip fracture? Psychogeriatrics. 2014; 14(2):118-23. [DOI:10.1111/psyg.12049] [PMID]
- Phillips AC, Upton J, Duggal NA, Carroll D, Lord JM. Depression following hip fracture is associated with increased physical frailty in older adults: The role of the cortisol: Dehydroepiandrosterone sulphate ratio. BMC Geriatr. 2013; 13:60. [DOI:10.1186/1471-2318-13-60] [PMID]
- Rathbun AM, Shardell M, Orwig D, Gruber-Baldini AL, Ostir G, Hicks GE, et al. Effects of prefracture depressive illness and postfracture depressive symptoms on physical performance after hip fracture. J Am Geriatr Soc. 2016; 64(11):e171-6. [DOI:10.1111/jgs.14487]
- Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: A preliminary report. J Psychiatr Res. 1982-1983; 17(1):37-49. [DOI:10.1016/0022-3956(82)90033-4] [PMID]
- Beaupre LA, Binder EF, Cameron ID, Jones CA, Orwig D, Sherrington C, et al. Maximising functional recovery following hip fracture in frail seniors. Best Pract Res Clin Rheumatol. 2013; 27(6):771-88. [DOI:10.1016/j.berh.2014.01.001] [PMID]
- Alexopoulos GS. Depression in the elderly. Lancet. 2005; 365(9475):1961-70. [DOI:10.1016/S0140-6736(05)66665-2] [PMID]
- Luppa M, Sikorski C, Luck T, Ehreke L, Konnopka A, Wiese B, et al. Age- and gender-specific prevalence of depression in latest-life--systematic review and meta-analysis. J Affect Disord. 2012; 136(3):212-21. [DOI:10.1016/j.jad.2010.11.033] [PMID]
- Vaughan L, Corbin AL, Goveas JS. Depression and frailty in later life: A systematic review. Clin Interv Aging. 2015; 10:1947-58. [DOI:10.2147/CIA.S69632]
- Young Y, Fried LP, Kuo YH. Hip fractures among elderly women: longitudinal comparison of physiological function changes and health care utilization. J Am Med Dir Assoc. 2010; 11(2):100-5. [DOI:10.1016/j.jamda.2009.09.005]
- Cole MG, Dendukuri N. Risk factors for depression among elderly community subjects: A systematic review and meta-analysis. Am J Psychiatry. 2003; 160(6):1147-56. [DOI:10.1176/appi.ajp.160.6.1147] [PMID]
- Kim SY, Lee JK, Oh DJ, Kong IG, Choi HG. Depression and incident hip fracture: A longitudinal follow-up study using a national sample cohort. Medicine (Baltimore). 2019; 98(26):e16268. [DOI:10.1097/MD.0000000000016268] [PMID]
- Radinovic K, Milan Z, Markovic-Denic L, Dubljanin-Raspopovic E, Jovanovic B, Bumbasirevic V. Predictors of severe pain in the immediate postoperative period in elderly patients following hip fracture surgery. Injury. 2014; 45(8):1246-50. [DOI:10.1016/j.injury.2014.05.024] [PMID]
- Radinovic KS, Markovic-Denic L, Dubljanin-Raspopovic E, Marinkovic J, Jovanovic LB, Bumbasirevic V. Effect of the overlap syndrome of depressive symptoms and delirium on outcomes in elderly adults with hip fracture: A prospective cohort study. J Am Geriatr Soc. 2014; 62(9):1640-8.[DOI:10.1111/jgs.12992]
- Sterling RS. Gender and race/ethnicity differences in hip fracture incidence, morbidity, mortality, and function. Clin Orthop Relat Res. 2011; 469(7):1913-8. [DOI:10.1007/s11999-010-1736-3] [PMID]
- Shyu YI, Cheng HS, Teng HC, Chen MC, Wu CC, Tsai WC. Older people with hip fracture: Depression in the postoperative first year. J Adv Nurs. 2009; 65(12):2514-22. [DOI:10.1111/j.1365-2648.2009.05125.x]
- Lebe M, Hasenbring MI, Schmieder K, Jetschke K, Harders A, Epplen JT, et al. Association of serotonin-1A and -2A receptor promoter polymorphisms with depressive symptoms, functional recovery, and pain in patients 6 months after lumbar disc surgery. Pain. 2013; 154(3):377-84. [DOI:10.1016/j.pain.2012.11.017] [PMID]
- Geha PY, Baliki MN, Harden RN, Bauer WR, Parrish TB, Apkarian AV. The brain in chronic CRPS pain: Abnormal gray-white matter interactions in emotional and autonomic regions. Neuron. 2008; 60(4):570-81. [DOI:10.1016/j.neuron.2008.08.022]
- Kodama D, Ono H, Tanabe M. Altered hippocampal long-term potentiation after peripheral nerve injury in mice. Eur J Pharmacol. 2007; 574(2-3):127-32. [DOI:10.1016/j.ejphar.2007.07.054] [PMID]
- Voshaar RC, Banerjee S, Horan M, Baldwin R, Pendleton N, Proctor R, et al. Predictors of incident depression after hip fracture surgery. Am J Geriatr Psychiatry. 2007; 15(9):807-14. [DOI:10.1097/JGP.0b013e318098610c]
- Bruggemann L, Nixon RD, Cavenett T. Predicting acute anxiety and depression following hip fracture. J Behav Med. 2007; 30(2):97-105. [DOI:10.1007/s10865-006-9088-x] [PMID]
- Xiang X, Brooks J. Correlates of depressive symptoms among homebound and semi-homebound older adults. J Gerontol Soc Work. 2017; 60(3):201-14. [DOI:10.1080/01634372.2017.1286625]
- Fan XM, Bi ZG, Fu CJ, Wang XM, Zou JL, Chen HJ, et al. [Clinical study of psychological changes and post traumatic stress disorder in elderly patients with hip fracture (Chinese)]. Zhonghua Wai Ke Za Zhi. 2020; 58(3):209-12. [DOI: 10.3760/cma.j.issn.0529-5815.2020.03.008] [PMID]
- Liu HY, Yang CT, Tseng MY, Chen CY, Wu CC, Cheng HS, et al. Trajectories in postoperative recovery of elderly hip-fracture patients at risk for depression: A follow-up study. Rehabil Psychol. 2018; 63(3):438-46. [DOI:10.1037/rep0000130]
- Arabyat RM, Raisch DW. Relationships between social/emotional support and quality of life, depression and disability in patients with chronic obstructive pulmonary disease: An analysis based on propensity score matching. Ann Behav Med. 2019; 53(10):918-27. [DOI:10.1093/abm/kaz002] [PMID]
- Lorant V, Croux C, Weich S, Deliège D, Mackenbach J, Ansseau M. Depression and socio-economic risk factors: 7-year longitudinal population study. Br J Psychiatry. 2007; 190:293-8. [DOI:10.1192/bjp.bp.105.020040]
- Agarwal S, Germosen C, Kil N, Bucovsky M, Colon I, Williams J, et al. Current anti-depressant use is associated with cortical bone deficits and reduced physical function in elderly women. Bone. 2020; 140:115552. [DOI:10.1016/j.bone.2020.115552]
- Wu Q. Depression and antidepressant medications: Both are linked to increased fracture risk. Osteoporos Int. 2019; 30(3):695-6. [DOI:10.1007/s00198-018-4785-1]
- Power C, Duffy R, Mahon J, McCarroll K, Lawlor BA. Bones of Contention: A comprehensive literature review of Non-SSRI Antidepressant Use and Bone Health. J Geriatr Psychiatry Neurol. 2020; 33(6):340-52. [DOI:10.1177/0891988719882091]
Type of Study: Research Article |
Subject:
Hip surgery
Received: 2025/02/4 | Accepted: 2024/05/13 | Published: 2024/05/1
Received: 2025/02/4 | Accepted: 2024/05/13 | Published: 2024/05/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
