

Volume 12, Issue 1 (Winter 2025)
JROS 2025, 12(1): 65-70 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gharanizadeh K, Yahyazadeh H, Aminian A, Amiri S, Zareie B, Sajedi S et al . Cephalomedullary Nail Versus Dynamic Hip Screw-plate Fixation: A Comparative Analysis of Ipsilateral Femoral Neck and Shaft Fracture Outcomes. JROS 2025; 12 (1) :65-70
URL: http://jros.iums.ac.ir/article-1-2292-en.html
URL: http://jros.iums.ac.ir/article-1-2292-en.html
Kaveh Gharanizadeh1 

 , Hooman Yahyazadeh2 , Amir Aminian1 , Shayan Amiri3 , Bushra Zareie1 , Saeedehsadat Sajedi4 , Sajad Noorigaravand1
, Hooman Yahyazadeh2 , Amir Aminian1 , Shayan Amiri3 , Bushra Zareie1 , Saeedehsadat Sajedi4 , Sajad Noorigaravand1
, Hooman Yahyazadeh2 , Amir Aminian1 , Shayan Amiri3 , Bushra Zareie1 , Saeedehsadat Sajedi4 , Sajad Noorigaravand1
1- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. & Department of Orthopedic, TMC.C, Islamic Azad University, Tehran, Iran.
3- Department of Orthopaedic, School of Medicine, Hazrat-Rasul Hospital, Iran University of Medical Sciences, Tehran, Iran.
4- Department of Orthopedic, TMC.C, Islamic Azad University, Tehran, Iran. & Department of Orthopedic Surgery, Farhikhtegan Hospital, Islamic Azad University, Tehran, Iran.
2- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. & Department of Orthopedic, TMC.C, Islamic Azad University, Tehran, Iran.
3- Department of Orthopaedic, School of Medicine, Hazrat-Rasul Hospital, Iran University of Medical Sciences, Tehran, Iran.
4- Department of Orthopedic, TMC.C, Islamic Azad University, Tehran, Iran. & Department of Orthopedic Surgery, Farhikhtegan Hospital, Islamic Azad University, Tehran, Iran.
Keywords: Ipsilateral femoral neck and shaft fracture, Cephalomedullary nail (CMN), Dynamic hip screw (DHS), Avascular necrosis (AVN), Fracture non:union:, Revision surgery, Smoking, Internal fixation
Full-Text [PDF 481 kb]
(151 Downloads)
| Abstract (HTML) (504 Views)
Full-Text: (131 Views)
Introduction
Ipsilateral fractures of the femoral neck and shaft represent a rare but serious injury pattern, typically resulting from high-energy trauma such as motor vehicle accidents or falls from height. These complex injuries are most commonly seen in young adults and are associated with significant morbidity if not managed appropriately [1]. Due to the anatomical and biomechanical differences between the femoral neck and shaft, treating both fractures simultaneously poses a unique surgical challenge.
The optimal fixation method for these dual fractures remains controversial. Two primary surgical strategies have been proposed: The use of a single cephalomedullary nail (CMN) that spans from the femoral head to the shaft, and a dual-implant technique involving separate fixation devices—typically a dynamic hip screw (DHS) for the neck and a plate for the shaft [2, 3]. Each approach has its advantages and limitations. CMN allows for a minimally invasive, time-efficient procedure and preserves soft tissues; however, it may compromise stability at one fracture site, particularly if the neck and shaft fractures are not aligned in a favorable configuration [4]. In contrast, the dual-implant technique offers tailored stabilization for each fracture but may be associated with longer operative times and greater blood loss [3].
Despite multiple biomechanical and clinical studies, there is still no consensus on which approach yields superior outcomes for fracture :union:, risk of avascular necrosis (AVN) of the femoral head, and the need for revision surgery. Moreover, patient-related factors such as age, smoking status, and gender may further influence healing potential and complicate treatment decisions [5, 6].
Given these uncertainties, this retrospective study compared the clinical outcomes of CMN fixation with DHS and plate fixation in patients with ipsilateral femoral neck and shaft fractures. Specifically, we aimed to analyze rates of fracture :union:, AVN, and revision surgery, while also assessing the impact of patient-related risk factors. The findings of this study may help inform surgical decision-making and identify high-risk patients who require closer monitoring and tailored intervention.
Methods
This retrospective study included 33 patients presenting with simultaneous fractures of the femoral neck and shaft. The management of these combined fractures remains a subject of debate, particularly whether both fractures should be stabilized with a single fixation device or treated with separate implants. Accordingly, the patients were divided into two groups for comparison: One group underwent fixation of both fractures with a single CMN, while the second group received dual fixation with a proximal device for the femoral neck and a separate plate for the femoral shaft. Outcomes assessed included fracture :union: rates, incidence of AVN, and the need for revision surgery. These parameters were compared between the two groups.
Results
In this study, 33 patients with simultaneous femoral neck and shaft fractures, with a Mean±SD age of 35.97±10.16 years, who underwent surgical treatment, were evaluated. More than 80% of the patients were male, while approximately 20% were female. Nearly 45% of these patients required revision surgery. The Mean±SD age of those who underwent revision surgery was 37.47±11.64 years, compared to 34.72±8.88 years for those who did not require additional surgery. Approximately 25% of patients developed AVN of the femoral head following surgery. The patients’ smoking status and type of fixation device used are presented in Table 1.

Bivariate analyses examining associations between various factors and outcomes, including fracture :union:, AVN, and revision surgery, are summarized in Table 2.
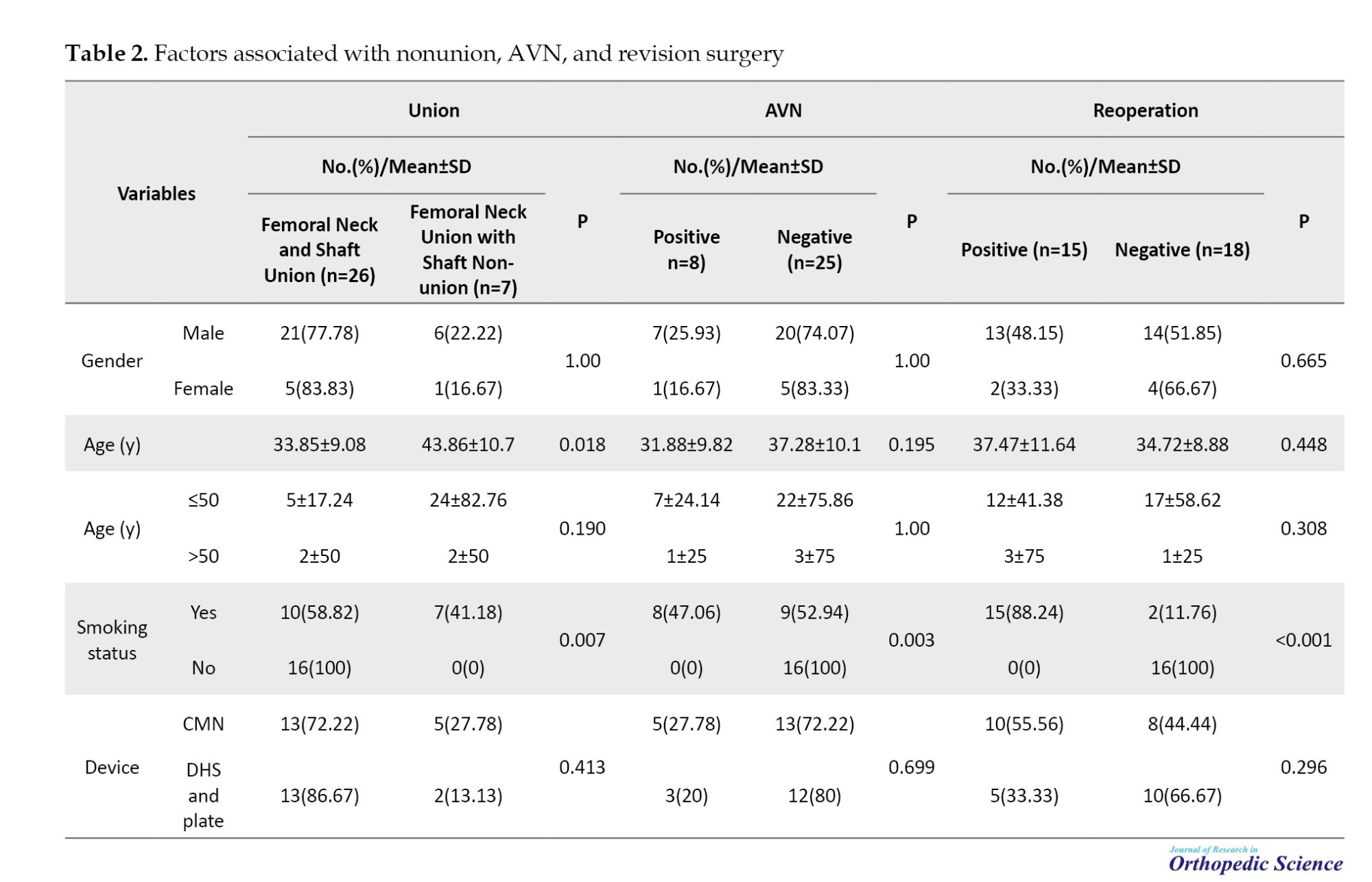
The mean age of patients experiencing non:union: of the femoral shaft was significantly higher—by about 10 years—compared to those with complete :union: of both the femoral neck and shaft fractures (43.86 vs 33.85 years). All non-smoking patients achieved complete :union: of the femoral neck and shaft postoperatively, whereas 41% of smokers developed femoral shaft non:union: following surgery. Similarly, 47% of smokers experienced postoperative AVN of the femoral head (P=0.007), whereas none were observed among non-smokers (P=0.003). Consistent with these findings, 88% of smokers required revision surgery, whereas none of the non-smoking patients needed additional surgical intervention (P<0.001).
The relationships between age, gender, smoking status, and fixation device type and fracture :union: were analyzed using logistic regression in both unadjusted and adjusted models; the results are presented in Table 3.
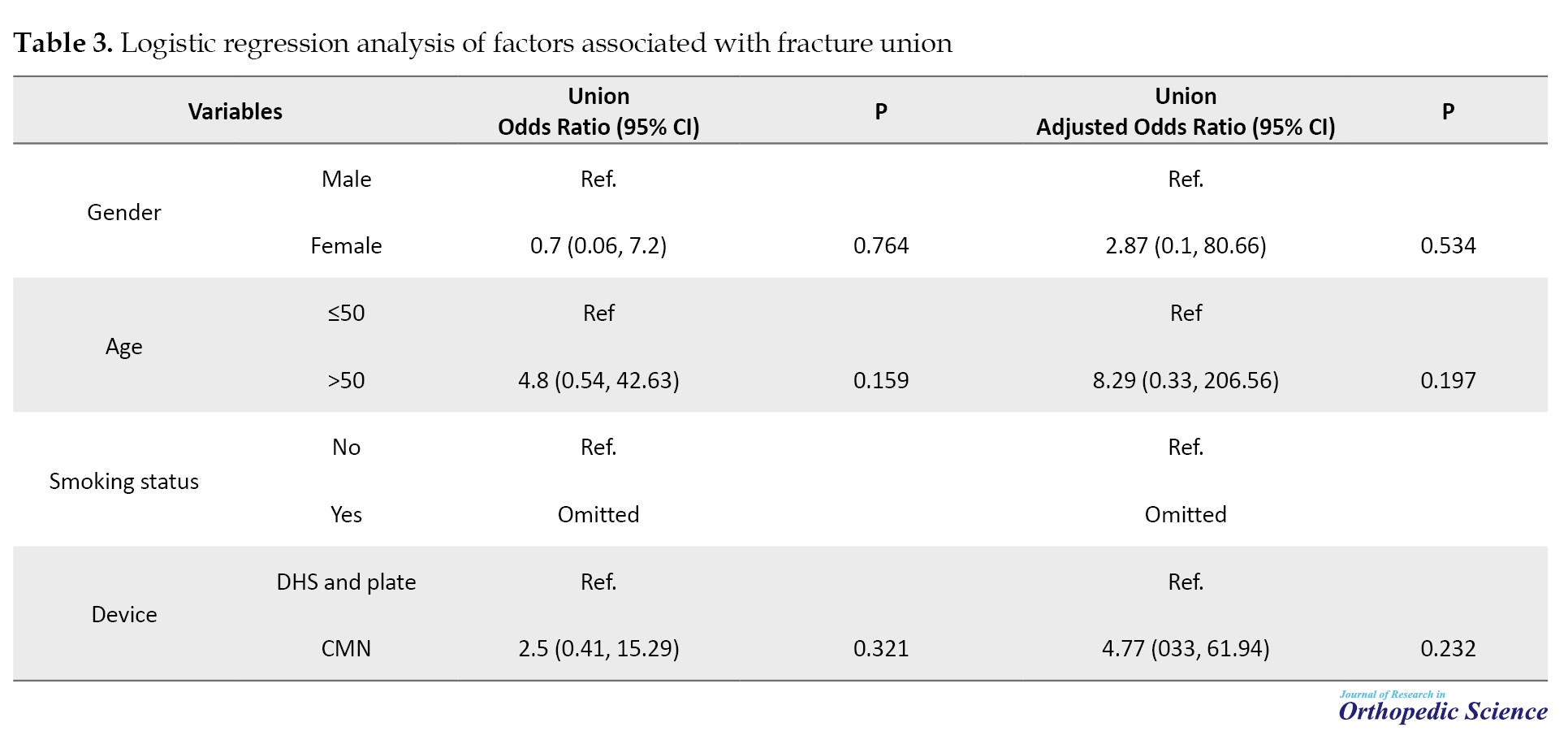
In univariate analysis, the odds of femoral shaft non:union: were 2.5 (95% CI, 0.41%, 15.29%) times higher in patients treated with cephalomedullary nailing than in those fixed with DHS and a plate. After adjusting for age, sex, and smoking status, the odds ratio increased to 4.77 (95% CI: 0.37%, 61.94%). Patients over 50 years old had an 8.29-fold higher risk of femoral shaft non:union: compared to those under 50, assuming other factors were held constant (Table 3). Additionally, the odds of non:union: in females were 2.87 times greater than in males.
Discussion
The treatment of simultaneous ipsilateral femoral neck and shaft fractures remains a surgical dilemma. While the use of a single CMN offers advantages such as reduced operative time and less soft-tissue disruption, concerns persist regarding its biomechanical limitations—particularly its ability to provide optimal stability at both fracture sites when they are non-colinear [3, 2].
In the present study, although both fixation methods demonstrated reasonable outcomes, the dual-implant approach (DHS for the neck and a plate for the shaft) showed a trend toward better :union: rates and fewer complications, especially in high-risk patients. This result is consistent with the findings of Watson et al. (2002), who reported that dual fixation provides improved alignment and reduced rates of non:union: and AVN in similar fracture patterns [3].
Our results also indicated a higher, though statistically nonsignificant, risk of femoral shaft non:union: with CMN fixation. This observation is in line with the study by Jain et al. (2004), who found that CMN may not provide adequate fixation in certain complex shaft fractures, particularly when the entry point compromises the neck fragment’s stability [2].
Interestingly, smoking was found to be a significant predictor of adverse outcomes. All patients who developed AVN or required revision surgery were smokers. Previous studies have shown a clear link between tobacco use and impaired revascularization of the femoral head, as well as diminished bone healing capacity, both of which contribute to an increased risk of postoperative complications [7].
Another noteworthy finding was an increased risk of non:union: in older patients, particularly those aged 50 or older. This finding aligns with prior studies emphasizing that age-related reductions in bone density and regenerative capacity adversely affect fracture healing [8].
From a biomechanical perspective, Ricci et al. highlighted the limitations of intramedullary nails in controlling torsional and axial forces across multiple fracture sites, especially when the medullary canal anatomy varies significantly between proximal and distal segments [9]. Our findings support these concerns, as CMN fixation was associated with a non:union: odds ratio nearly 5 times that of the dual-implant group in the adjusted analysis.
Sex-related differences in outcomes were observed but not statistically significant. However, further research with larger sample sizes is needed to understand better the potential influence of gender on bone healing and implant-related outcomes.
Taken together, our study reinforces the importance of individualized treatment planning. Factors such as patient age, smoking status, and fracture geometry should guide the choice of fixation method. While CMN may be suitable for select low-risk patients, dual fixation may offer superior outcomes in more complex or high-risk cases.
Conclusion
In conclusion, this study found that smoking and older age are major risk factors for adverse outcomes—including fracture non:union:, AVN, and need for revision surgery—following surgical treatment of ipsilateral femoral neck and shaft fractures. While both fixation methods (CMN and DHS with plate) demonstrated acceptable clinical outcomes, the dual-implant approach may be associated with fewer complications in selected patients. Importantly, smoking cessation and careful preoperative risk stratification are essential components of management. Future prospective multicenter studies with larger sample sizes are needed to validate these findings and refine treatment guidelines for this challenging fracture pattern.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of Tehran Medical Sciences Branch, Islamic Azad University, Tehran, Iran (Code: IR.IAU.TMU.REC.1403.019).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Ipsilateral fractures of the femoral neck and shaft represent a rare but serious injury pattern, typically resulting from high-energy trauma such as motor vehicle accidents or falls from height. These complex injuries are most commonly seen in young adults and are associated with significant morbidity if not managed appropriately [1]. Due to the anatomical and biomechanical differences between the femoral neck and shaft, treating both fractures simultaneously poses a unique surgical challenge.
The optimal fixation method for these dual fractures remains controversial. Two primary surgical strategies have been proposed: The use of a single cephalomedullary nail (CMN) that spans from the femoral head to the shaft, and a dual-implant technique involving separate fixation devices—typically a dynamic hip screw (DHS) for the neck and a plate for the shaft [2, 3]. Each approach has its advantages and limitations. CMN allows for a minimally invasive, time-efficient procedure and preserves soft tissues; however, it may compromise stability at one fracture site, particularly if the neck and shaft fractures are not aligned in a favorable configuration [4]. In contrast, the dual-implant technique offers tailored stabilization for each fracture but may be associated with longer operative times and greater blood loss [3].
Despite multiple biomechanical and clinical studies, there is still no consensus on which approach yields superior outcomes for fracture :union:, risk of avascular necrosis (AVN) of the femoral head, and the need for revision surgery. Moreover, patient-related factors such as age, smoking status, and gender may further influence healing potential and complicate treatment decisions [5, 6].
Given these uncertainties, this retrospective study compared the clinical outcomes of CMN fixation with DHS and plate fixation in patients with ipsilateral femoral neck and shaft fractures. Specifically, we aimed to analyze rates of fracture :union:, AVN, and revision surgery, while also assessing the impact of patient-related risk factors. The findings of this study may help inform surgical decision-making and identify high-risk patients who require closer monitoring and tailored intervention.
Methods
This retrospective study included 33 patients presenting with simultaneous fractures of the femoral neck and shaft. The management of these combined fractures remains a subject of debate, particularly whether both fractures should be stabilized with a single fixation device or treated with separate implants. Accordingly, the patients were divided into two groups for comparison: One group underwent fixation of both fractures with a single CMN, while the second group received dual fixation with a proximal device for the femoral neck and a separate plate for the femoral shaft. Outcomes assessed included fracture :union: rates, incidence of AVN, and the need for revision surgery. These parameters were compared between the two groups.
Results
In this study, 33 patients with simultaneous femoral neck and shaft fractures, with a Mean±SD age of 35.97±10.16 years, who underwent surgical treatment, were evaluated. More than 80% of the patients were male, while approximately 20% were female. Nearly 45% of these patients required revision surgery. The Mean±SD age of those who underwent revision surgery was 37.47±11.64 years, compared to 34.72±8.88 years for those who did not require additional surgery. Approximately 25% of patients developed AVN of the femoral head following surgery. The patients’ smoking status and type of fixation device used are presented in Table 1.
Bivariate analyses examining associations between various factors and outcomes, including fracture :union:, AVN, and revision surgery, are summarized in Table 2.
The mean age of patients experiencing non:union: of the femoral shaft was significantly higher—by about 10 years—compared to those with complete :union: of both the femoral neck and shaft fractures (43.86 vs 33.85 years). All non-smoking patients achieved complete :union: of the femoral neck and shaft postoperatively, whereas 41% of smokers developed femoral shaft non:union: following surgery. Similarly, 47% of smokers experienced postoperative AVN of the femoral head (P=0.007), whereas none were observed among non-smokers (P=0.003). Consistent with these findings, 88% of smokers required revision surgery, whereas none of the non-smoking patients needed additional surgical intervention (P<0.001).
The relationships between age, gender, smoking status, and fixation device type and fracture :union: were analyzed using logistic regression in both unadjusted and adjusted models; the results are presented in Table 3.
In univariate analysis, the odds of femoral shaft non:union: were 2.5 (95% CI, 0.41%, 15.29%) times higher in patients treated with cephalomedullary nailing than in those fixed with DHS and a plate. After adjusting for age, sex, and smoking status, the odds ratio increased to 4.77 (95% CI: 0.37%, 61.94%). Patients over 50 years old had an 8.29-fold higher risk of femoral shaft non:union: compared to those under 50, assuming other factors were held constant (Table 3). Additionally, the odds of non:union: in females were 2.87 times greater than in males.
Discussion
The treatment of simultaneous ipsilateral femoral neck and shaft fractures remains a surgical dilemma. While the use of a single CMN offers advantages such as reduced operative time and less soft-tissue disruption, concerns persist regarding its biomechanical limitations—particularly its ability to provide optimal stability at both fracture sites when they are non-colinear [3, 2].
In the present study, although both fixation methods demonstrated reasonable outcomes, the dual-implant approach (DHS for the neck and a plate for the shaft) showed a trend toward better :union: rates and fewer complications, especially in high-risk patients. This result is consistent with the findings of Watson et al. (2002), who reported that dual fixation provides improved alignment and reduced rates of non:union: and AVN in similar fracture patterns [3].
Our results also indicated a higher, though statistically nonsignificant, risk of femoral shaft non:union: with CMN fixation. This observation is in line with the study by Jain et al. (2004), who found that CMN may not provide adequate fixation in certain complex shaft fractures, particularly when the entry point compromises the neck fragment’s stability [2].
Interestingly, smoking was found to be a significant predictor of adverse outcomes. All patients who developed AVN or required revision surgery were smokers. Previous studies have shown a clear link between tobacco use and impaired revascularization of the femoral head, as well as diminished bone healing capacity, both of which contribute to an increased risk of postoperative complications [7].
Another noteworthy finding was an increased risk of non:union: in older patients, particularly those aged 50 or older. This finding aligns with prior studies emphasizing that age-related reductions in bone density and regenerative capacity adversely affect fracture healing [8].
From a biomechanical perspective, Ricci et al. highlighted the limitations of intramedullary nails in controlling torsional and axial forces across multiple fracture sites, especially when the medullary canal anatomy varies significantly between proximal and distal segments [9]. Our findings support these concerns, as CMN fixation was associated with a non:union: odds ratio nearly 5 times that of the dual-implant group in the adjusted analysis.
Sex-related differences in outcomes were observed but not statistically significant. However, further research with larger sample sizes is needed to understand better the potential influence of gender on bone healing and implant-related outcomes.
Taken together, our study reinforces the importance of individualized treatment planning. Factors such as patient age, smoking status, and fracture geometry should guide the choice of fixation method. While CMN may be suitable for select low-risk patients, dual fixation may offer superior outcomes in more complex or high-risk cases.
Conclusion
In conclusion, this study found that smoking and older age are major risk factors for adverse outcomes—including fracture non:union:, AVN, and need for revision surgery—following surgical treatment of ipsilateral femoral neck and shaft fractures. While both fixation methods (CMN and DHS with plate) demonstrated acceptable clinical outcomes, the dual-implant approach may be associated with fewer complications in selected patients. Importantly, smoking cessation and careful preoperative risk stratification are essential components of management. Future prospective multicenter studies with larger sample sizes are needed to validate these findings and refine treatment guidelines for this challenging fracture pattern.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of Tehran Medical Sciences Branch, Islamic Azad University, Tehran, Iran (Code: IR.IAU.TMU.REC.1403.019).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
- Alho A. Concurrent ipsilateral fractures of the hip and femoral shaft: A meta-analysis of 659 cases. Acta Orthop Scand. 1996; 67(1):19-28. [DOI:10.3109/17453679608995603] [PMID]
- Jain P, Maini L, Mishra P, Upadhyay A, Agarwal A. Cephalomedullary interlocked nail for ipsilateral hip and femoral shaft fractures. Injury. 2004; 35(10):1031-8. [DOI:10.1016/j.injury.2003.09.039] [PMID]
- Watson JT, Moed BR. Ipsilateral femoral neck and shaft fractures: Complications and their treatment. Clin Orthop Relat Res. 2002; (399):78-86. [DOI:10.1097/00003086-200206000-00011] [PMID]
- Jain R, Koo M, Kreder HJ, Schemitsch EH, Davey JR, Mahomed NN. Comparison of early and delayed fixation of subcapital hip fractures in patients sixty years of age or less. J Bone Joint Surg Am. 2002; 84(9):1605-12. [DOI:10.2106/00004623-200209000-00013] [PMID]
- Wang WT, Li YQ, Guo YM, Li M, Mei HB, Shao JF, et al. Risk factors for the development of avascular necrosis after femoral neck fractures in children: A review of 239 cases. Bone Joint J. 2019; 101-B(9):1160-7. [DOI:10.1302/0301-620X.101B9.BJJ-2019-0275.R1] [PMID]
- Parker MJ, Gurusamy K. Internal fixation versus arthroplasty for intracapsular proximal femoral fractures in adults. Cochrane Database Syst Rev. 2006; 2006(4):CD001708.[DOI:10.1002/14651858.CD001708.pub2] [PMID]
- Nishijima A, Yamamoto N, Yanagibayashi S, Yoshida R, Takikawa M, Kouno R, et al. The effect of smoking on necrosis rate in digital replantation and revascularization with prostaglandin E1 Therapy: A retrospective study. Plast Reconstr Surg. 2016; 138(4):848-53. [DOI:10.1097/PRS.0000000000002600] [PMID]
- Gómez Alonso C, Díaz Curiel M, Hawkins Carranza F, Pérez Cano R, Díez Pérez A; Multicenter Project for Research in Osteoporosis. Femoral bone mineral density, neck-shaft angle and mean femoral neck width as predictors of hip fracture in men and women. Osteoporos Int. 2000; 11(8):714-20. [DOI:10.1007/s001980070071] [PMID]
- Ricci WM, Gallagher B, Haidukewych GJ. Intramedullary nailing of femoral shaft fractures: Current concepts. J Am Acad Orthop Surg. 2009; 17(5):296-305. [DOI:10.5435/00124635-200905000-00004] [PMID]
Type of Study: Research Article |
Subject:
Hip surgery
Received: 2024/11/3 | Accepted: 2024/12/21 | Published: 2025/02/1
Received: 2024/11/3 | Accepted: 2024/12/21 | Published: 2025/02/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
