

Volume 12, Issue 2 (Spring 2025)
JROS 2025, 12(2): 103-106 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nakhaei Amroodi M, Bahaeddini M, Khajeh Alizadeh Attarr M, Hashemipour B, Mahdavifar M, Tabrizian P. Atypical Terrible Triad Injuries of the Elbow Associated With Triceps Tendon Avulsion: A Case Series. JROS 2025; 12 (2) :103-106
URL: http://jros.iums.ac.ir/article-1-2302-en.html
URL: http://jros.iums.ac.ir/article-1-2302-en.html
Atypical Terrible Triad Injuries of the Elbow Associated With Triceps Tendon Avulsion: A Case Series
Morteza Nakhaei Amroodi1 

 , Mohammadreza Bahaeddini1 , Mojtaba Khajeh Alizadeh Attarr1 , Babak Hashemipour1 , Mohammadmehdi Mahdavifar1 , Pouria Tabrizian1
, Mohammadreza Bahaeddini1 , Mojtaba Khajeh Alizadeh Attarr1 , Babak Hashemipour1 , Mohammadmehdi Mahdavifar1 , Pouria Tabrizian1
, Mohammadreza Bahaeddini1 , Mojtaba Khajeh Alizadeh Attarr1 , Babak Hashemipour1 , Mohammadmehdi Mahdavifar1 , Pouria Tabrizian1
1- Bone and Joint Reconstruction Research Center, School of Medicine, Shafayahyaeian Hospital, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 815 kb]
(93 Downloads)
| Abstract (HTML) (287 Views)
Full-Text: (62 Views)
Introduction
The terrible triad injury of the elbow was first introduced by Hotchkiss in 1966 and is defined by the presence of elbow dislocation or subluxation accompanied by fractures of the coronoid process and the radial head [1]. Notably, rupture of the triceps tendon is not considered part of the classical description of this injury pattern [2]. Terrible triad injuries are associated with a wide spectrum of complications, including nerve damage, wound-healing problems, heterotopic ossification, joint stiffness, non:union:, mal:union:, infection, and persistent instability [3, 4]. Given the highly congruent nature of the elbow joint, even minimal residual incongruity can adversely affect joint function and lead to unfavorable clinical outcomes [5].
With advances in surgical techniques and an improved understanding of elbow biomechanics, functional outcomes have significantly improved; nevertheless, deviations from the classic definition of the terrible triad are being increasingly reported in the literature [6, 7].
The purpose of this case series was to describe four patients with atypical terrible triad injuries of the elbow associated with triceps tendon avulsion and to highlight diagnostic considerations and surgical management strategies.
Case Presentation
This case series includes four patients diagnosed with atypical terrible triad injuries of the elbow. Demographic data, mechanism of injury, associated lesions, surgical treatment, and clinical parameters are summarized in Table 1.
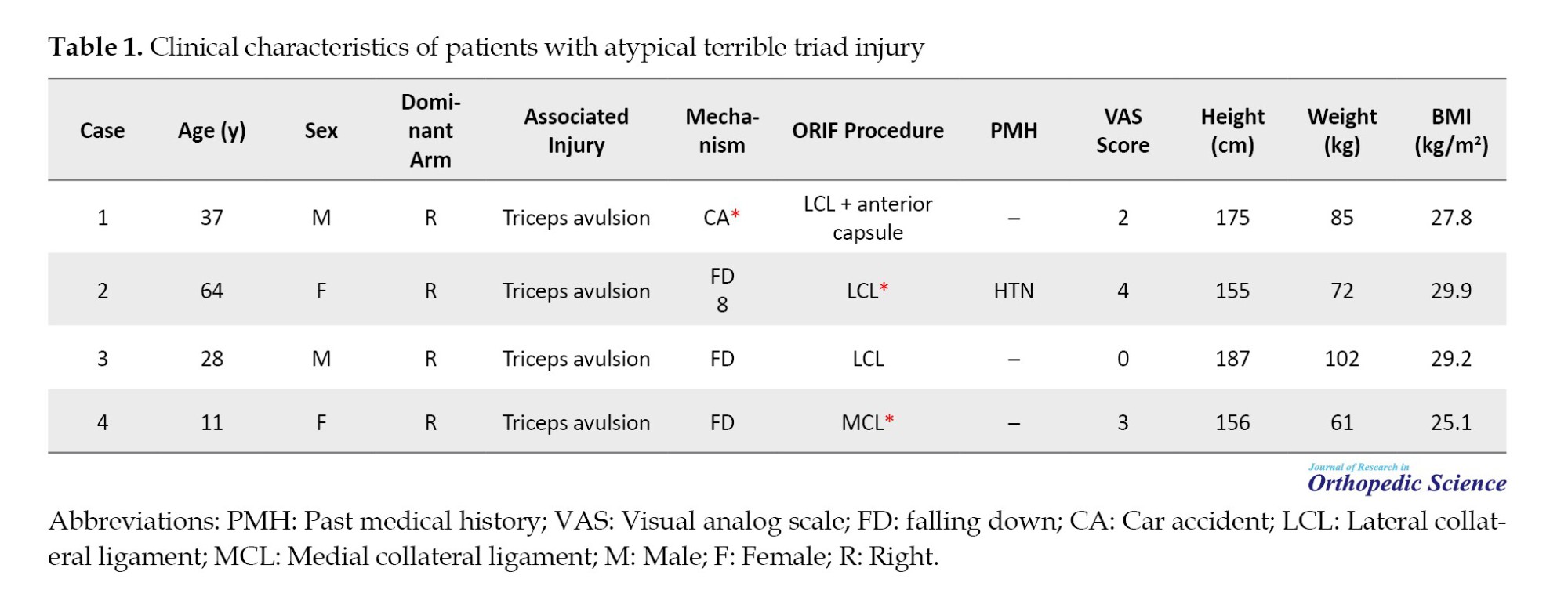
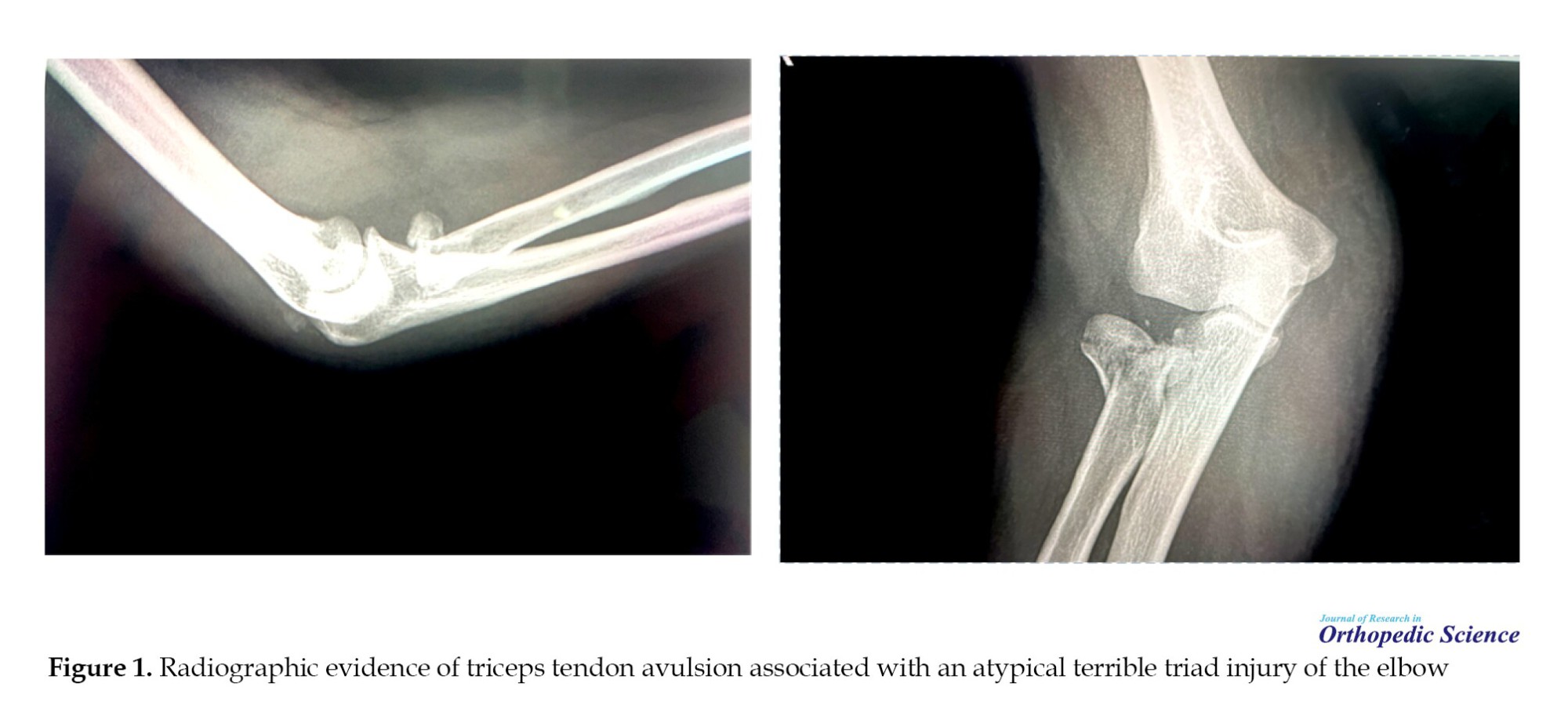
All patients presented with acute elbow trauma accompanied by fracture–dislocation. Radiographic evaluation confirmed radial head involvement in all cases, along with elbow dislocation and associated triceps tendon avulsion. The mechanism of injury was falling down in three patients and car accident in one patient. One patient had a medical history of hypertension.
Surgical treatment consisted of open reduction and internal fixation (ORIF) tailored to fracture configuration, including management of the lateral collateral ligament and anterior capsule when indicated. Postoperative protocols emphasized early controlled mobilization to prevent stiffness while maintaining joint stability.
Discussion
Accurate preoperative diagnosis of triceps tendon rupture in the setting of terrible triad elbow injuries remains challenging. Due to pain, swelling, and gross instability, reliable clinical assessment of elbow extension strength is often not feasible in the acute phase. Consequently, diagnosis frequently depends on radiologic findings rather than physical examination.
One important radiographic indicator of triceps avulsion is the so-called “flake sign,” which appears as a small avulsed bony fragment from the olecranon, representing the insertion site of the triceps tendon [6]. Recognition of this subtle finding is critical, as failure to identify triceps involvement may lead to underestimation of elbow instability. However, it should be noted that triceps ruptures do not always demonstrate a visible flake sign on standard radiographs [3-5].
Although magnetic resonance imaging (MRI) can provide detailed evaluation of soft tissue injuries, its routine use in all patients with terrible triad injuries may not be cost-effective or practical, particularly in the acute trauma setting [3-5]. Similar diagnostic difficulties have been described in other complex joint injuries, such as rotator cuff tears associated with shoulder fracture–dislocations or patellar tendon ruptures occurring with knee dislocations [8].
These complex injury patterns require a comprehensive diagnostic approach that integrates clinical suspicion with careful interpretation of imaging studies [9-11]. When a triceps tendon avulsion is suspected or confirmed, early and appropriate surgical intervention is essential to prevent long-term complications, such as persistent instability, weakness in elbow extension, and poor functional outcomes [4, 5, 11, 12].
Surgical repair of the triceps tendon is crucial to restoring posterior stability of the elbow and maintaining functional joint mechanics. In cases of atypical terrible triad injuries, instability is often more severe than that observed in classical terrible triad patterns, emphasizing the need for meticulous surgical planning and complete soft-tissue reconstruction [12].
Additionally, previous studies have shown that radial head resection may yield acceptable outcomes in selected terrible triad cases, provided that the interosseous membrane remains intact and an adequate range of motion is preserved postoperatively [13]. This highlights the importance of individualized treatment strategies based on the overall stability of the elbow rather than adherence to a single fixed surgical algorithm.
Conclusion
Atypical terrible triad injuries of the elbow associated with triceps tendon avulsion represent a rare and complex injury pattern. Awareness of this variant, careful imaging assessment, and individualized surgical management are essential to achieve satisfactory clinical outcomes.
Ethical Considerations
Compliance with ethical guidelines
Informed consent was obtained from the patients for the publication of this case report.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
The terrible triad injury of the elbow was first introduced by Hotchkiss in 1966 and is defined by the presence of elbow dislocation or subluxation accompanied by fractures of the coronoid process and the radial head [1]. Notably, rupture of the triceps tendon is not considered part of the classical description of this injury pattern [2]. Terrible triad injuries are associated with a wide spectrum of complications, including nerve damage, wound-healing problems, heterotopic ossification, joint stiffness, non:union:, mal:union:, infection, and persistent instability [3, 4]. Given the highly congruent nature of the elbow joint, even minimal residual incongruity can adversely affect joint function and lead to unfavorable clinical outcomes [5].
With advances in surgical techniques and an improved understanding of elbow biomechanics, functional outcomes have significantly improved; nevertheless, deviations from the classic definition of the terrible triad are being increasingly reported in the literature [6, 7].
The purpose of this case series was to describe four patients with atypical terrible triad injuries of the elbow associated with triceps tendon avulsion and to highlight diagnostic considerations and surgical management strategies.
Case Presentation
This case series includes four patients diagnosed with atypical terrible triad injuries of the elbow. Demographic data, mechanism of injury, associated lesions, surgical treatment, and clinical parameters are summarized in Table 1.
All patients presented with acute elbow trauma accompanied by fracture–dislocation. Radiographic evaluation confirmed radial head involvement in all cases, along with elbow dislocation and associated triceps tendon avulsion. The mechanism of injury was falling down in three patients and car accident in one patient. One patient had a medical history of hypertension.
Surgical treatment consisted of open reduction and internal fixation (ORIF) tailored to fracture configuration, including management of the lateral collateral ligament and anterior capsule when indicated. Postoperative protocols emphasized early controlled mobilization to prevent stiffness while maintaining joint stability.
Discussion
Accurate preoperative diagnosis of triceps tendon rupture in the setting of terrible triad elbow injuries remains challenging. Due to pain, swelling, and gross instability, reliable clinical assessment of elbow extension strength is often not feasible in the acute phase. Consequently, diagnosis frequently depends on radiologic findings rather than physical examination.
One important radiographic indicator of triceps avulsion is the so-called “flake sign,” which appears as a small avulsed bony fragment from the olecranon, representing the insertion site of the triceps tendon [6]. Recognition of this subtle finding is critical, as failure to identify triceps involvement may lead to underestimation of elbow instability. However, it should be noted that triceps ruptures do not always demonstrate a visible flake sign on standard radiographs [3-5].
Although magnetic resonance imaging (MRI) can provide detailed evaluation of soft tissue injuries, its routine use in all patients with terrible triad injuries may not be cost-effective or practical, particularly in the acute trauma setting [3-5]. Similar diagnostic difficulties have been described in other complex joint injuries, such as rotator cuff tears associated with shoulder fracture–dislocations or patellar tendon ruptures occurring with knee dislocations [8].
These complex injury patterns require a comprehensive diagnostic approach that integrates clinical suspicion with careful interpretation of imaging studies [9-11]. When a triceps tendon avulsion is suspected or confirmed, early and appropriate surgical intervention is essential to prevent long-term complications, such as persistent instability, weakness in elbow extension, and poor functional outcomes [4, 5, 11, 12].
Surgical repair of the triceps tendon is crucial to restoring posterior stability of the elbow and maintaining functional joint mechanics. In cases of atypical terrible triad injuries, instability is often more severe than that observed in classical terrible triad patterns, emphasizing the need for meticulous surgical planning and complete soft-tissue reconstruction [12].
Additionally, previous studies have shown that radial head resection may yield acceptable outcomes in selected terrible triad cases, provided that the interosseous membrane remains intact and an adequate range of motion is preserved postoperatively [13]. This highlights the importance of individualized treatment strategies based on the overall stability of the elbow rather than adherence to a single fixed surgical algorithm.
Conclusion
Atypical terrible triad injuries of the elbow associated with triceps tendon avulsion represent a rare and complex injury pattern. Awareness of this variant, careful imaging assessment, and individualized surgical management are essential to achieve satisfactory clinical outcomes.
Ethical Considerations
Compliance with ethical guidelines
Informed consent was obtained from the patients for the publication of this case report.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
- Hotchkiss RN. Fractures and dislocations of the elbow. Fractures in adults. Pennsylvania: Lippincott-Raven; 1996. [Link]
- Ebrahimzadeh MH, Amadzadeh-Chabock H, Ring D. Traumatic elbow instability. J Hand Surg Am. 2010; 35(7):1220-5. [DOI:10.1016/j.jhsa.2010.05.002] [PMID]
- Dodds SD, Fishler T. Terrible triad of the elbow. Orthop Clin North Am. 2013; 44(1):47-58. [DOI:10.1016/j.ocl.2012.08.006] [PMID]
- Mathew PK, Athwal GS, King GJ. Terrible triad injury of the elbow: Current concepts. J Am Acad Orthop Surg. 2009; 17(3):137-51. [DOI:10.5435/00124635-200903000-00003] [PMID]
- Ring D, Jupiter JB, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am. 2002; 84(4):547-51. [DOI:10.2106/00004623-200204000-00006] [PMID]
- Anakwe RE, Middleton SD, Jenkins PJ, McQueen MM. Patient-reported outcomes after simple dislocation of the elbow. J Bone Joint Surg Am. 2011; 93(13):1220-6. [DOI:10.2106/JBJS.J.00860] [PMID]
- van der Horst AS, Stephens AR, Wei G, Presson AP, Tashjian RZ, Kazmers NH. Prognostic factors affecting long-term outcomes after elbow dislocation: A longitudinal cohort study. J Hand Surg Glob Online. 2021; 3(5):260-5. [DOI:10.1016/j.jhsg.2021.05.011] [PMID]
- Dehghani Nazhvani H, Bemani Lirgeshasi S, Bahari M. Terrible triad elbow fracture dislocation with ipsilateral triceps avulsion and radial shaft fracture: A case report. JBJS Case Connect. 2020; 10(4):e20.00308. [DOI:10.2106/JBJS.CC.20.00308] [PMID]
- Garrigues GE, Wray WH 3rd, Lindenhovius AL, Ring DC, Ruch DS. Fixation of the coronoid process in elbow fracture-dislocations. J Bone Joint Surg Am. 2011; 93(20):1873-81. [DOI:10.2106/JBJS.I.01673] [PMID]
- Leigh WB, Ball CM. Radial head reconstruction versus replacement in the treatment of terrible triad injuries of the elbow. J Shoulder Elbow Surg. 2012; 21(10):1336-41. [DOI:10.1016/j.jse.2012.03.005] [PMID]
- Rodriguez-Martin J, Pretell-Mazzini J, Andres-Esteban EM, Larrainzar-Garijo R. Outcomes after terrible triads of the elbow treated with the current surgical protocols. A review. Int Orthop. 2011; 35(6):851-60. [DOI:10.1007/s00264-010-1024-6] [PMID]
- Lindenhovius AL, Jupiter JB, Ring D. Comparison of acute versus subacute treatment of terrible triad injuries of the elbow. J Hand Surg Am. 2008; 33(6):920-6. [DOI:10.1016/j.jhsa.2008.02.007] [PMID]
- Najd MF, Shariatzadeh H, Sadony H, Bagheri N, Ebrahimy H. Comparison of radial head resection with radial head fixation in the terrible triad injury of the elbow. J Res Orthop Sci. 2019; 6(4):19-24. [Link]
Type of Study: Case Report |
Subject:
Shoulder / Elbow
Received: 2025/01/15 | Accepted: 2025/03/21 | Published: 2025/05/1
Received: 2025/01/15 | Accepted: 2025/03/21 | Published: 2025/05/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
