

Volume 12, Issue 3 (Summer 2025)
JROS 2025, 12(3): 145-150 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kargar Shooroki K, Hajialiloo Sami S, hamidzadeh Khiavi A, moazen A, barati Y, roshanravan B. Osteosarcoma of the Distal Radius Treated by Wide Resection and Reconstruction With a Vascularized Fibular Graft: A Case Report. JROS 2025; 12 (3) :145-150
URL: http://jros.iums.ac.ir/article-1-2304-en.html
URL: http://jros.iums.ac.ir/article-1-2304-en.html
Khalil Kargar Shooroki1 

 , Sam Hajialiloo Sami1 , Amin Hamidzadeh Khiavi1 , Alireza Moazen1 , Yousef Barati1 , Babak Roshanravan2
, Sam Hajialiloo Sami1 , Amin Hamidzadeh Khiavi1 , Alireza Moazen1 , Yousef Barati1 , Babak Roshanravan2
, Sam Hajialiloo Sami1 , Amin Hamidzadeh Khiavi1 , Alireza Moazen1 , Yousef Barati1 , Babak Roshanravan2
1- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. & Department of Orthopedics, School of Medicine, Shafayahyaeian Hospital, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. & Department of Orthopedics, School of Medicine, Shafayahyaeian Hospital, Iran University of Medical Sciences, Tehran, Iran. & Geriatric Health Research Center, Birjand University of Medical Sciences, Birjand, Iran.
2- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. & Department of Orthopedics, School of Medicine, Shafayahyaeian Hospital, Iran University of Medical Sciences, Tehran, Iran. & Geriatric Health Research Center, Birjand University of Medical Sciences, Birjand, Iran.
Keywords: Osteosarcoma, Distal Radius, Vascularized fibular graft, Biological reconstruction, Limb-salvage surgery, Bone tumor reconstruction
Full-Text [PDF 3395 kb]
(104 Downloads)
| Abstract (HTML) (304 Views)
Full-Text: (51 Views)
Introduction
The present study discussed the use of vascularized fibular grafts in reconstructing skeletal defects after the excision of bone tumors. Osteosarcoma is the most common primary malignant bone tumor with unclear origin, typically presenting in the second decade of life [1]. While the distal radius is a relatively common area for primary bone tumors, osteosarcoma in this location is uncommon; fewer than 1% of osteosarcomas arise in the distal radius [2]. Tumors of the distal radius present challenges because of their anatomy, histological type, tumor size, and potential mechanical dysfunction of the elbow or hand joint [3]. Described procedures include arthrodesis ulnar translocation, osteoarticular allograft, using bulk autograft, reconstruction with vascularized or non-vascularized fibular grafts, and prosthetic replacement [2-4]. Free vascularized fibular transfer can aid in rapid autograft incorporation in limbs affected by radiation or adjuvant chemotherapy [5]. Free vascularized fibular transfer offers the potential for rapid autograft incorporation in limbs affected by adjuvant chemotherapy or radiation. In the upper extremity, the fibula’s tubular shape and easy access to recipient vessels render it one of the most promising areas for free fibular transfer. The fibula’s size and contour closely resemble the radius and ulna diaphyses, making it an appropriate donor for reconstruction of substantial forearm bone loss. Such similarities mostly enable vascularized fibula reconstruction to produce a stable wrist and forearm [6-8]. Vascularized bone grafts (VBGs) have facilitated reconstruction of upper-extremity defects by offering superior regenerative capacity compared with non-vascularized grafts, the ability to repair large bone defects, and multiple donor-site options. VBGs can be used as pedicled or free transfers and may enable composite tissue transfers when both bone and soft tissue reconstruction are required [5]. This article reviews the use of vascularized fibular grafts in skeletal reconstruction, emphasizing long-term outcomes and improvements in patients’ quality of life.
Case Presentation
Medical history
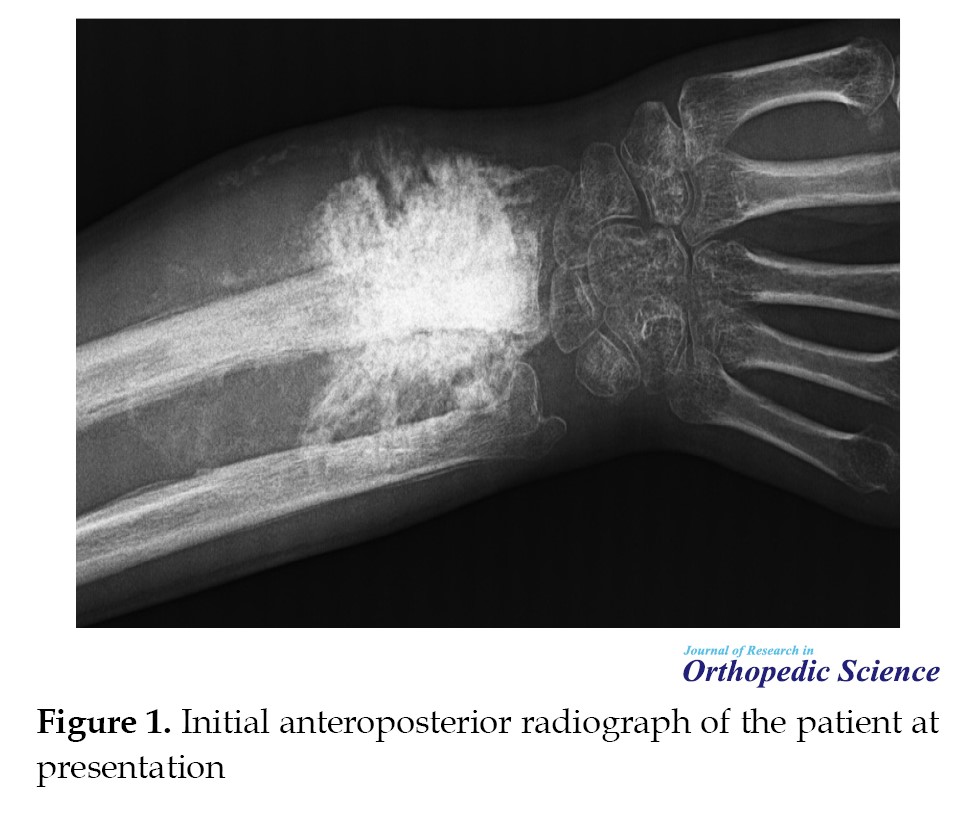
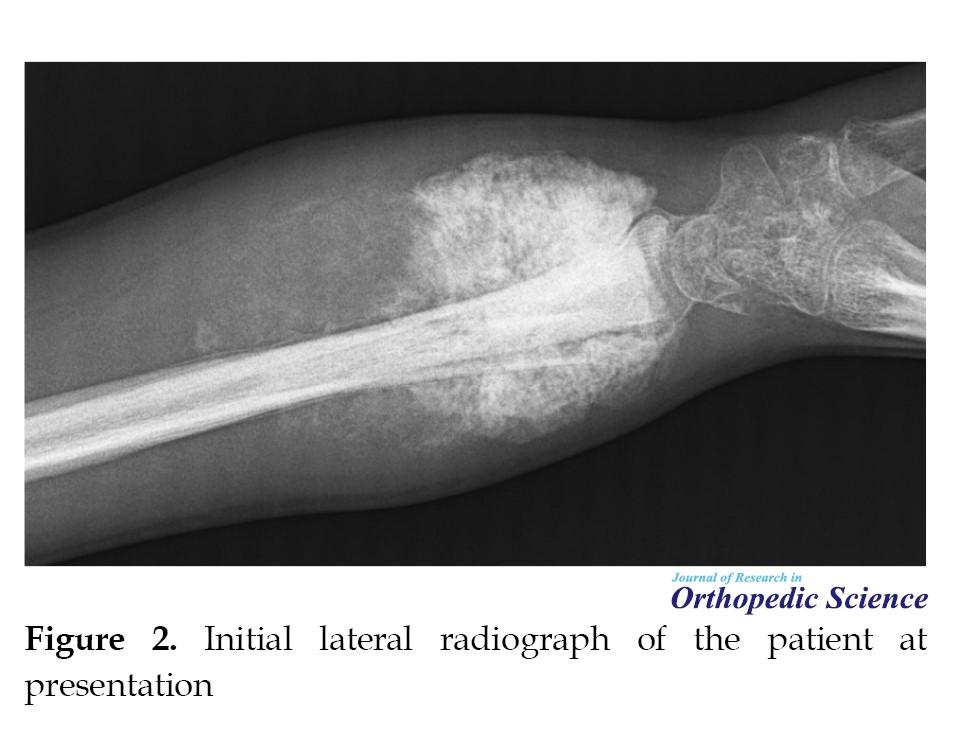
A 20-year-old male farmer with no significant medical history presented with progressive pain, swelling, and deformity of the right wrist. Physical examination revealed a hard, irregular mass on the dorsal and volar aspects of the distal radius, severe tenderness, reduced wrist range of motion, and decreased hand grip strength. Initial radiographs demonstrated a lytic lesion with indistinct margins and a permeative pattern extending beyond the bone (Figures 1 and 2).
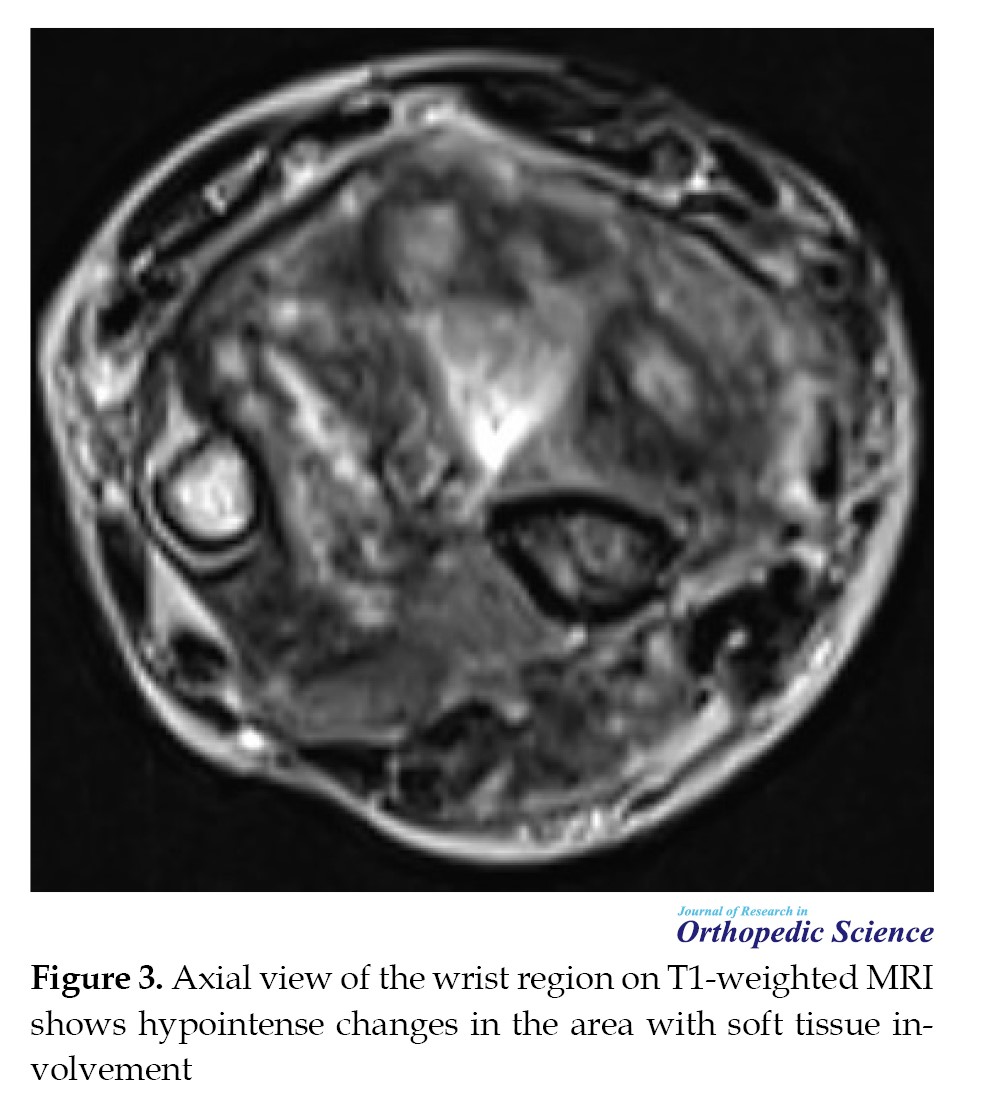
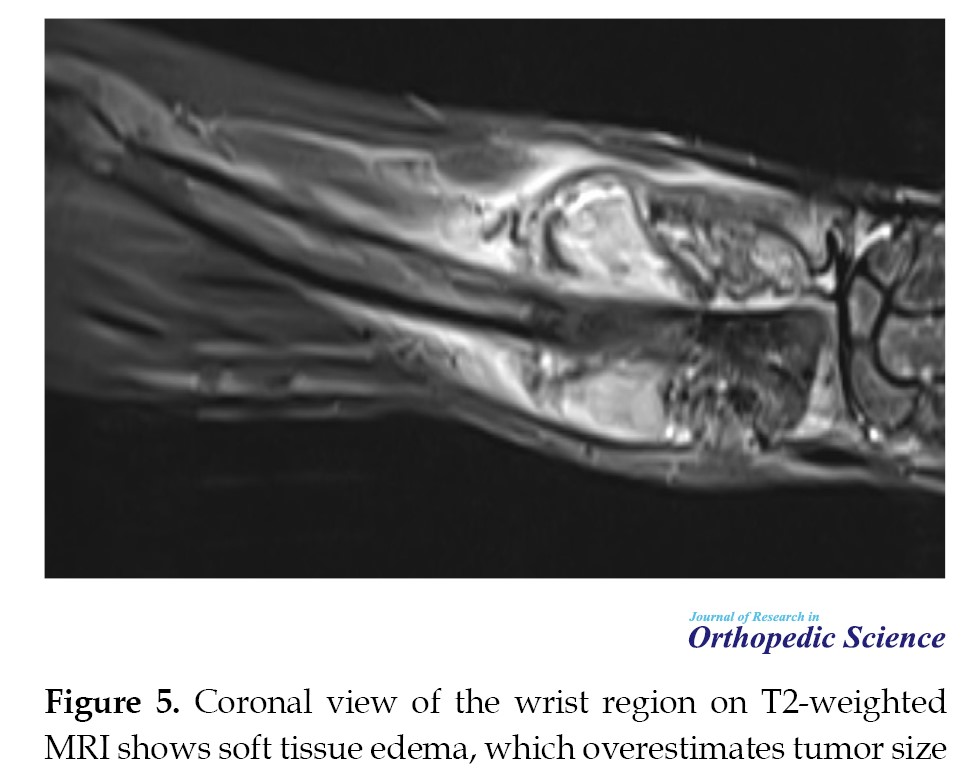
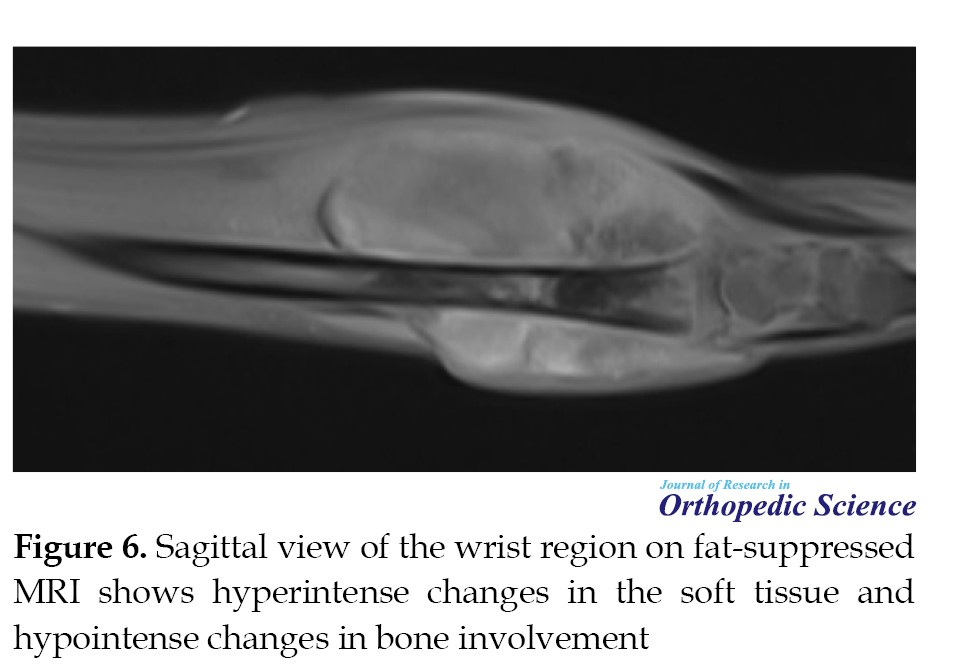
 Magnetic resonance imaging (MRI) showed a hypointense lesion on T1-weighted images and a hyperintense lesion on T2-weighted and fat-suppressed images, with soft tissue extension (Figures 3, 4, 5 and 6).
Magnetic resonance imaging (MRI) showed a hypointense lesion on T1-weighted images and a hyperintense lesion on T2-weighted and fat-suppressed images, with soft tissue extension (Figures 3, 4, 5 and 6).

 Technetium-99 m scintigraphy revealed increased uptake within the lesion, whereas chest CT scan showed no evidence of metastasis. Laboratory investigations, including blood counts, C-reactive protein (CRP), sedimentation rate (ESR), and alkaline phosphatase, were within normal limits. Core needle biopsy confirmed osteosarcoma. The patient underwent five cycles of neoadjuvant chemotherapy at three-week intervals before definitive wide resection and reconstruction with a vascularized fibular graft.
Technetium-99 m scintigraphy revealed increased uptake within the lesion, whereas chest CT scan showed no evidence of metastasis. Laboratory investigations, including blood counts, C-reactive protein (CRP), sedimentation rate (ESR), and alkaline phosphatase, were within normal limits. Core needle biopsy confirmed osteosarcoma. The patient underwent five cycles of neoadjuvant chemotherapy at three-week intervals before definitive wide resection and reconstruction with a vascularized fibular graft.
Operative technique
The patient was placed under general anesthesia, and the surgical site was prepared and disinfected. A longitudinal dorsal incision at the radiocarpal joint was made to approach the distal radius, and an elliptical excision was performed at the previous biopsy site. The tumor, involving both radius and ulna, was resected with wide margins, and the involved nerves were sacrificed.
Simultaneously, a vascularized fibular graft was harvested in a bloodless field, preserving a muscle cuff and the peroneal vessels up to their trifurcation. To minimize ischemic time, vessels were not divided until the recipient site was prepared. The graft was fixed proximally with a plate and distally to the metacarpal with a pin, and the ulna was stabilized intramedullary. End-to-end microvascular anastomoses were performed between graft and recipient vessels. The wound was closed in layers, and the limb was immobilized in a splint. Surgical margins were sent for histopathological evaluation. The incision healed without complications.
Postoperative care
Histopathological examination of the resected specimens confirmed tumor-free surgical margins. Two weeks after surgery, the patient received six cycles of adjuvant chemotherapy at three-week intervals, following the same regimen as preoperative therapy, and tolerated the treatment well. Informed consent for surgery and postoperative care was obtained from the patient and his family.
Results and follow-up
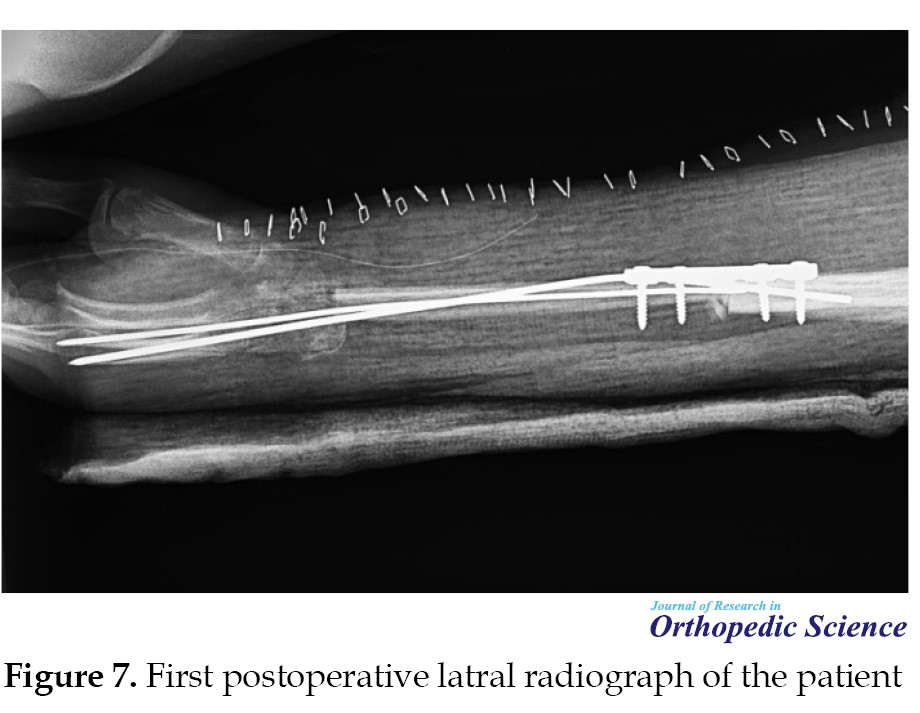
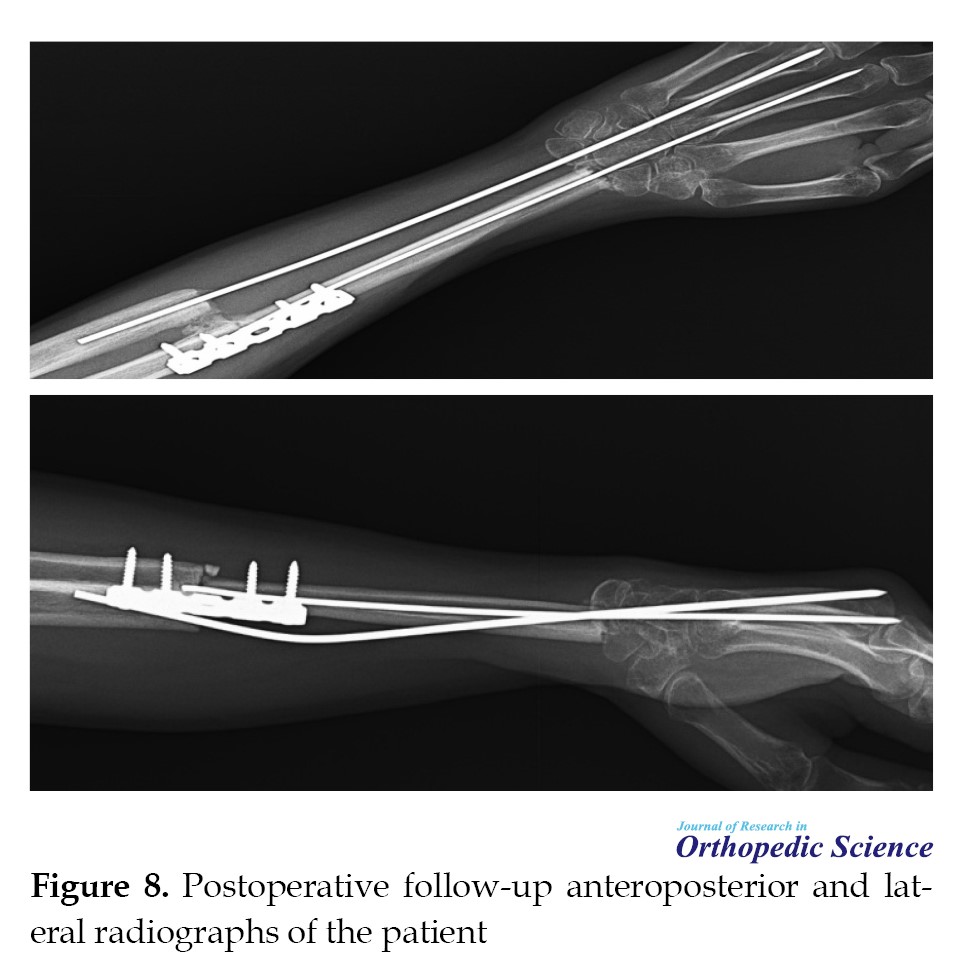
Postoperative radiographs (Figures 7, 8, and 9) demonstrated satisfactory graft placement and evidence of callus formation at the graft-host junction.
 The patient’s wrist and fingers were initially immobilized in a splint, with gentle mobilization exercises started to prevent stiffness. Physiotherapy was continued to restore hand grip strength and functional use. At one-month follow-up, there was no wrist deformity, instability, metastasis, or local recurrence. Pronation and supination were slightly limited due to injury to the posterior interosseous nerve (PIN); movements in the PIN innervation zone were lost. Despite this, the patient performed daily activities independently and reported satisfaction with functional outcomes. At final evaluation, complete bone graft :union: was confirmed, with no signs of infection or tumor recurrence. Vascularized bone grafts demonstrated robust healing and functional recovery, consistent with their ability to tolerate mechanical stress, even in patients receiving chemotherapy or radiotherapy.
The patient’s wrist and fingers were initially immobilized in a splint, with gentle mobilization exercises started to prevent stiffness. Physiotherapy was continued to restore hand grip strength and functional use. At one-month follow-up, there was no wrist deformity, instability, metastasis, or local recurrence. Pronation and supination were slightly limited due to injury to the posterior interosseous nerve (PIN); movements in the PIN innervation zone were lost. Despite this, the patient performed daily activities independently and reported satisfaction with functional outcomes. At final evaluation, complete bone graft :union: was confirmed, with no signs of infection or tumor recurrence. Vascularized bone grafts demonstrated robust healing and functional recovery, consistent with their ability to tolerate mechanical stress, even in patients receiving chemotherapy or radiotherapy.
Discussion
Osteosarcoma of the distal radius is extremely rare, and reconstruction following wide resection is technically demanding given limited soft tissue and complex biomechanics. Previous reports have documented various options, such as prosthesis, allografts, non-vascularized and vascularized fibular grafts for distal radius reconstruction after tumor excision, but very few specifically report osteosarcoma in this location [2]. Free vascularized fibular grafting offers viable biological reconstruction with living osteocytes and osteoblasts that facilitate primary healing and structural stability in large defects of the forearm and upper extremity [9]. Published studies have shown high :union: rates for free vascularized fibular grafts in forearm reconstruction, with many series reporting reliable graft consolidation and functional outcomes [9]. Comparisons in the literature further demonstrate improved :union: and reduced complications with vascularized grafts compared with non-vascularized techniques for major skeletal reconstructions [10]. In extremity osteosarcoma reconstructions, vascularized fibular grafts have been applied successfully with satisfactory healing and functional outcomes across multiple sites [11]. In our case, the patient achieved complete graft :union: and was able to perform daily activities independently despite adjuvant chemotherapy, which corroborates the growing evidence that vascularized fibular grafts are a reliable option in complex oncologic reconstructions.
Conclusion
Free vascularized fibular grafting represents a reliable biological reconstruction technique for large skeletal defects following distal radius osteosarcoma resection. In this case, the procedure resulted in complete graft :union:, preserved wrist stability, and satisfactory functional recovery despite adjuvant chemotherapy. Vascularized fibular grafts provide durable structural support and acceptable functional outcomes, making them a valuable limb-salvage option in complex oncologic reconstructions of the upper extremity.
Ethical Considerations
Compliance with ethical guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Khalil Kargar Shuraki, Sami Sam Hajialiloo, Babak Roshanravan and Alireza Moazen; Surgery and data collection: Amin Hamidzadeh Khiavi, Yousef Barati; Data analysis: Khalil Kargar Shuraki and Sami Sam Hajialiloo; Writing the original draft: Amin Hamidzadeh Khiavi, Yousef Barati, Khalil Kargar Shuraki and Sami Sam Hajialiloo; Supervision, review and editing: Babak Roshanravan and Alireza Moazen.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors gratefully acknowledge the contributions of all the patients who participated in this study, as well as the surgeons, nurses, and medical staff involved in surgery and postoperative care provided. Special thanks to the multidisciplinary teams whose collaboration made the comprehensive management of these complex cases possible.
References
The present study discussed the use of vascularized fibular grafts in reconstructing skeletal defects after the excision of bone tumors. Osteosarcoma is the most common primary malignant bone tumor with unclear origin, typically presenting in the second decade of life [1]. While the distal radius is a relatively common area for primary bone tumors, osteosarcoma in this location is uncommon; fewer than 1% of osteosarcomas arise in the distal radius [2]. Tumors of the distal radius present challenges because of their anatomy, histological type, tumor size, and potential mechanical dysfunction of the elbow or hand joint [3]. Described procedures include arthrodesis ulnar translocation, osteoarticular allograft, using bulk autograft, reconstruction with vascularized or non-vascularized fibular grafts, and prosthetic replacement [2-4]. Free vascularized fibular transfer can aid in rapid autograft incorporation in limbs affected by radiation or adjuvant chemotherapy [5]. Free vascularized fibular transfer offers the potential for rapid autograft incorporation in limbs affected by adjuvant chemotherapy or radiation. In the upper extremity, the fibula’s tubular shape and easy access to recipient vessels render it one of the most promising areas for free fibular transfer. The fibula’s size and contour closely resemble the radius and ulna diaphyses, making it an appropriate donor for reconstruction of substantial forearm bone loss. Such similarities mostly enable vascularized fibula reconstruction to produce a stable wrist and forearm [6-8]. Vascularized bone grafts (VBGs) have facilitated reconstruction of upper-extremity defects by offering superior regenerative capacity compared with non-vascularized grafts, the ability to repair large bone defects, and multiple donor-site options. VBGs can be used as pedicled or free transfers and may enable composite tissue transfers when both bone and soft tissue reconstruction are required [5]. This article reviews the use of vascularized fibular grafts in skeletal reconstruction, emphasizing long-term outcomes and improvements in patients’ quality of life.
Case Presentation
Medical history
A 20-year-old male farmer with no significant medical history presented with progressive pain, swelling, and deformity of the right wrist. Physical examination revealed a hard, irregular mass on the dorsal and volar aspects of the distal radius, severe tenderness, reduced wrist range of motion, and decreased hand grip strength. Initial radiographs demonstrated a lytic lesion with indistinct margins and a permeative pattern extending beyond the bone (Figures 1 and 2).
Operative technique
The patient was placed under general anesthesia, and the surgical site was prepared and disinfected. A longitudinal dorsal incision at the radiocarpal joint was made to approach the distal radius, and an elliptical excision was performed at the previous biopsy site. The tumor, involving both radius and ulna, was resected with wide margins, and the involved nerves were sacrificed.
Simultaneously, a vascularized fibular graft was harvested in a bloodless field, preserving a muscle cuff and the peroneal vessels up to their trifurcation. To minimize ischemic time, vessels were not divided until the recipient site was prepared. The graft was fixed proximally with a plate and distally to the metacarpal with a pin, and the ulna was stabilized intramedullary. End-to-end microvascular anastomoses were performed between graft and recipient vessels. The wound was closed in layers, and the limb was immobilized in a splint. Surgical margins were sent for histopathological evaluation. The incision healed without complications.
Postoperative care
Histopathological examination of the resected specimens confirmed tumor-free surgical margins. Two weeks after surgery, the patient received six cycles of adjuvant chemotherapy at three-week intervals, following the same regimen as preoperative therapy, and tolerated the treatment well. Informed consent for surgery and postoperative care was obtained from the patient and his family.
Results and follow-up
Postoperative radiographs (Figures 7, 8, and 9) demonstrated satisfactory graft placement and evidence of callus formation at the graft-host junction.
Discussion
Osteosarcoma of the distal radius is extremely rare, and reconstruction following wide resection is technically demanding given limited soft tissue and complex biomechanics. Previous reports have documented various options, such as prosthesis, allografts, non-vascularized and vascularized fibular grafts for distal radius reconstruction after tumor excision, but very few specifically report osteosarcoma in this location [2]. Free vascularized fibular grafting offers viable biological reconstruction with living osteocytes and osteoblasts that facilitate primary healing and structural stability in large defects of the forearm and upper extremity [9]. Published studies have shown high :union: rates for free vascularized fibular grafts in forearm reconstruction, with many series reporting reliable graft consolidation and functional outcomes [9]. Comparisons in the literature further demonstrate improved :union: and reduced complications with vascularized grafts compared with non-vascularized techniques for major skeletal reconstructions [10]. In extremity osteosarcoma reconstructions, vascularized fibular grafts have been applied successfully with satisfactory healing and functional outcomes across multiple sites [11]. In our case, the patient achieved complete graft :union: and was able to perform daily activities independently despite adjuvant chemotherapy, which corroborates the growing evidence that vascularized fibular grafts are a reliable option in complex oncologic reconstructions.
Conclusion
Free vascularized fibular grafting represents a reliable biological reconstruction technique for large skeletal defects following distal radius osteosarcoma resection. In this case, the procedure resulted in complete graft :union:, preserved wrist stability, and satisfactory functional recovery despite adjuvant chemotherapy. Vascularized fibular grafts provide durable structural support and acceptable functional outcomes, making them a valuable limb-salvage option in complex oncologic reconstructions of the upper extremity.
Ethical Considerations
Compliance with ethical guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Khalil Kargar Shuraki, Sami Sam Hajialiloo, Babak Roshanravan and Alireza Moazen; Surgery and data collection: Amin Hamidzadeh Khiavi, Yousef Barati; Data analysis: Khalil Kargar Shuraki and Sami Sam Hajialiloo; Writing the original draft: Amin Hamidzadeh Khiavi, Yousef Barati, Khalil Kargar Shuraki and Sami Sam Hajialiloo; Supervision, review and editing: Babak Roshanravan and Alireza Moazen.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors gratefully acknowledge the contributions of all the patients who participated in this study, as well as the surgeons, nurses, and medical staff involved in surgery and postoperative care provided. Special thanks to the multidisciplinary teams whose collaboration made the comprehensive management of these complex cases possible.
References
- Messerschmitt PJ, Garcia RM, Abdul-Karim FW, Greenfield EM, Getty PJ. Osteosarcoma. J Am Acad Orthop Surg. 2009; 17(8):515-27. [DOI:10.5435/00124635-200908000-00005] [PMID]
- Yu X. Osteosarcoma of the distal radius treated by en bloc resection and reconstruction with a fibular shaft preserving the radiocarpal joint: A case report. Oncol Lett. 2014; 7(5):1503-16. [DOI:10.3892/ol.2014.1891] [PMID]
- Clara-Altamirano MA, Luna-Ortiz K, Escobar-Alfaro G, Luna-Peteuil Z, Garcia-Ortega DY. Tumors of the proximal and distal radius with free fibular graft reconstruction. Ann Case Report. 2022; 7: 947. [DOI:10.29011/2574-7754.100947]
- Aithal V, Bhaskaranand K. Reconstruction of the distal radius by fibula following excision of giant cell tumor. Int Orthop. 2003; 27:110-3. [DOI:10.1007/s00264-002-0414-9] [PMID]
- Eward WC. Free vascularized fibular graft reconstruction of large skeletal defects after tumor resection. Clin Orthop Relat Res. 2010; 468(2):590-8. [DOI:10.1007/s11999-009-1053-x] [PMID]
- Sutanto P, Hamid A, Pradhana A. Excision of giant cell tumor followed by reconstruction of distal radius using free vascularized fibular graft. Neurologico Spinale Med Chirurgico. 2019; 1. [DOI:10.15562/nsmc.v1i4.134]
- Åberg M. Reconstruction with a free vascularized fibular graft for malignant bone tumor. Acta Orthop Scand. 1988; 59(4):430-7. [DOI:10.3109/17453678809149397] [PMID]
- Ceruso M, Falcone C, Innocenti M, Delcroix L, Capanna R, Manfrini M. Skeletal reconstruction with a free vascularized fibula graft associated to bone allograft after resection of malignant bone tumor of limbs. Handchir Mikrochir Plast Chir. 2001; 33(4):277-82. [DOI:10.1055/s-2001-16597] [PMID]
- Konstantinou P. Outcomes of free vascularized fibular grafts in treating massive forearm skeletal defects. J Per Med. 2024; 14(9):973. [DOI:10.3390/jpm14090973] [PMID]
- Thiel JT. A Treatment algorithm for free vascularized bone reconstruction in rare large osseous defects involving the wrist. Life. 2024; 14(9):1099. [DOI:10.3390/life14091099] [PMID]
- Xu L. Clinical outcome of free vascularized fibula graft in the surgical treatment of extremity osteosarcoma. Orthop Surg. 2020; 12(3):727-33. [DOI:10.1111/os.12646] [PMID]
Type of Study: Case Report |
Subject:
Tumor surgery
Received: 2025/01/13 | Accepted: 2025/05/21 | Published: 2025/08/1
Received: 2025/01/13 | Accepted: 2025/05/21 | Published: 2025/08/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
