

Volume 12, Issue 3 (Summer 2025)
JROS 2025, 12(3): 135-144 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bagherifard A, Jabalameli M, Askari A, Yahyazadeh H, Zareie B, Heidarikhoo M et al . Origin-specific Osteotomy for the Correction of Genu Valgum Deformity of the Knee: A Retrospective Study. JROS 2025; 12 (3) :135-144
URL: http://jros.iums.ac.ir/article-1-2306-en.html
URL: http://jros.iums.ac.ir/article-1-2306-en.html
Abolfazl Bagherifard1 

 , Mahmoud Jabalameli1 , Alireza Askari1 , Hooman Yahyazadeh2 , Bushra Zareie1 , Mohammadreza Heidarikhoo1 , Behnam Sour1
, Mahmoud Jabalameli1 , Alireza Askari1 , Hooman Yahyazadeh2 , Bushra Zareie1 , Mohammadreza Heidarikhoo1 , Behnam Sour1
, Mahmoud Jabalameli1 , Alireza Askari1 , Hooman Yahyazadeh2 , Bushra Zareie1 , Mohammadreza Heidarikhoo1 , Behnam Sour1
1- Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Orthopedics, TMS.C., Islamic Azad University, Tehran, Iran.
2- Department of Orthopedics, TMS.C., Islamic Azad University, Tehran, Iran.
Keywords: Genu valgum, Valgus deformity, Distal femoral osteotomy (DFO), Proximal tibial osteotomy (PTO), Long-leg radiographs, Joint-line orientation, Coronal realignment, Knee osteotomy
Full-Text [PDF 758 kb]
(76 Downloads)
| Abstract (HTML) (284 Views)
Full-Text: (44 Views)
Introduction
Valgus malalignment alters coronal-plane mechanics by shifting the mechanical axis laterally, increasing load across the lateral tibiofemoral compartment. In physiologically young adults with persistent symptoms, realignment osteotomy remains a dependable joint-preserving option. Its effectiveness, however, depends on correcting the deformity at the anatomical level responsible for the deviation. When correction is performed at the wrong segment, the mechanical axis may be restored, but the joint line can remain oblique, creating abnormal shear forces and compromising load distribution [1-3].
Distal femoral varus osteotomy (DFO) has historically been the standard treatment for symptomatic valgus deformity. Closing-wedge and, more recently, lateral opening-wedge techniques have produced reliable correction, solid :union:, and durable pain relief in several series, particularly when deformity originates in the distal femur [4-8]. However, detailed long-leg radiographic analysis has shown that valgus deformity does not always arise from the femur alone. Some patients demonstrate proximal tibial involvement, and others exhibit combined femoral, tibial, and intra-articular contributions [3, 9-11]. In such cases, a femur-only osteotomy may normalize the mechanical axis yet leave the joint line tilted.
Objective radiographic measures—the lateral distal femoral angle (LDFA), medial proximal tibial angle (MPTA), and joint-line convergence angle (JLCA)—provide a structured framework for identifying the anatomical source of deformity [1-3]. An origin-directed approach assigns the osteotomy to the segment demonstrating the primary deviation and uses double-level correction when both segments contribute substantially or when JLCA suggests an intra-articular component [12]. Although widely acknowledged conceptually, few clinical series have applied this strategy as a systematic decision algorithm.
The purpose of the present study was to evaluate an origin-specific approach to valgus realignment in adults. Deformities were classified by their anatomical origin using standardized long-leg radiographs, and patients underwent distal femoral, proximal tibial, or Double-level osteotomy (DLO) accordingly. We aimed to determine whether this strategy yields accurate coronal correction, preserves joint-line orientation, and produces satisfactory mid-term clinical outcomes.
Methods
Study design and ethical approval
This retrospective study was conducted at a tertiary orthopedic referral center. All adult patients who underwent realignment surgery for symptomatic valgus knee deformity between 2011 and 2018 were screened. The study protocol was approved by the institutional review board, and all participants provided informed consent.
Patient selection
Inclusion criteria were symptomatic coronal-plane valgus deformity confirmed on standing long-leg radiographs, age appropriate for joint-preserving surgery, and a minimum of two years of radiographic and clinical follow-up. Indications included lateral compartment pain related to valgus overload, progressive deformity, post-traumatic malalignment, ligamentous insufficiency with valgus thrust, neuromuscular sequelae, or early osteoarthritis in physiologically young adults.
Exclusion criteria were previous realignment surgery around the knee, metabolic bone disease, incomplete imaging, or inability to complete follow-up. Thirty-one patients (34 knees) met the criteria and were included.
Radiographic assessment
Standardized standing long-leg anteroposterior radiographs were obtained with the patella directed forward and both hips and ankles included. Imaging was performed under full weight-bearing. Measurements were performed digitally on PACS by the operating surgeon or a senior fellow.
Three parameters were assessed: LDFA, defined as the angle between the femoral mechanical axis and distal femoral joint line; MPTA, defined as the angle between the tibial mechanical axis and proximal tibial joint line; and JLCA, defined as the angle between the distal femoral and proximal tibial joint lines. Normal reference values (LDFA ≈ 87°, MPTA ≈ 87°, JLCA ≈ 0–2°) were used to determine deformity origin [1-3].
Classification of deformity origin
Deformities were classified as femoral-based, tibial-based, or combined deformities. This algorithm guided the selection of DFO, PTO, or DLO [1-3, 12].
Surgical techniques
Distal femoral osteotomy (DFO) was used for femoral-based deformity, typically employing a lateral opening-wedge technique. Through a lateral approach, the distal femur was exposed and a biplanar osteotomy created under fluoroscopic guidance, preserving a medial cortical hinge. The wedge was opened to the planned correction and fixed with a locking compression plate [4-8, 13-15].
Proximal tibial osteotomy (PTO) was used for tibial-based deformity. A medial approach was used to perform a medial opening- or closing-wedge osteotomy according to anatomy and surgeon preference, with careful preservation of posterior tibial slope [16, 17]. Fixation was achieved with a locking plate.
DLO was used for combined deformity or markedly increased JLCA. The correction magnitude was divided between distal femur and proximal tibia to maintain joint-line orientation while restoring the mechanical axis [3, 12].
Postoperative management
Passive and active-assisted motion began on the first postoperative day. The goal was to reach at least 90° of flexion by four weeks and a functional range of motion (ROM) by six weeks. Partial weight-bearing was initiated after early callus formation, typically at eight weeks, and progressed to full weight-bearing by ten to twelve weeks based on radiographic :union: and clinical tolerance.
Outcome measures
Radiographic outcomes included LDFA, MPTA, JLCA, and mechanical valgus angle, recorded preoperatively and at final follow-up. Clinical outcomes included knee ROM, Western Ontario and McMaster universities osteoarthritis index (WOMAC), and knee injury and osteoarthritis outcome score (KOOS). Validated Persian versions of WOMAC and KOOS were used when applicable [18-20]. Complications, such as non:union:, hardware irritation requiring removal, loss of correction, and recurrent valgus were recorded.
Statistical analysis
Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Preoperative and final follow-up values were compared using paired t-tests when normally distributed and non-parametric tests when appropriate. Categorical variables were compared using chi-square tests. Statistical significance was set at P<0.05.
Results
Thirty-one patients (34 knees) met the inclusion criteria. The cohort included 26 women (83.9%) and 5 men (16.1%), with a mean age of 34.8±9.9 years and a mean body mass index (BMI) of 23.3±2.9 kg/m². Mean follow-up duration was 4.2±2.7 years. Laterality was evenly distributed (14 right, 14 left), and three patients (9.6%) had bilateral procedures. Indications included valgus overload pain, progressive deformity, post-traumatic malalignment, ligamentous insufficiency with valgus thrust, neuromuscular conditions, and early osteoarthritis. Baseline characteristics are summarized in Table 1.

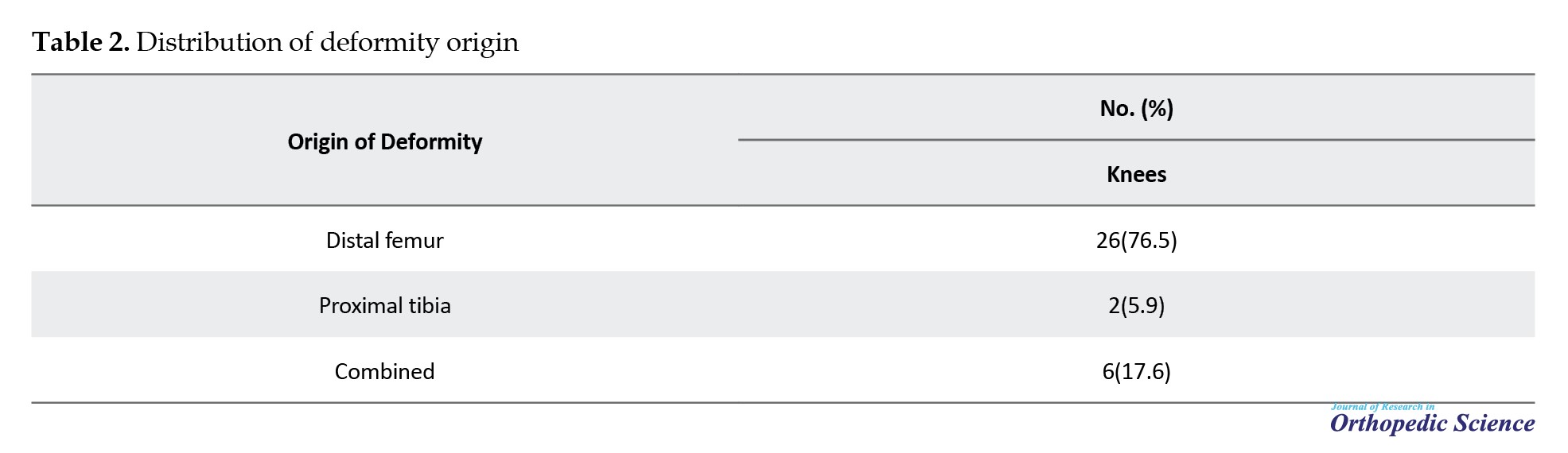
Radiographically, 26 knees (76.5%) showed femoral-based deformity, 2 knees (5.9%) had tibial-based deformity, and 6 knees (17.6%) had combined deformity or marked JLCA. The distribution of deformity origin is shown in Table 2 and Figure 1.
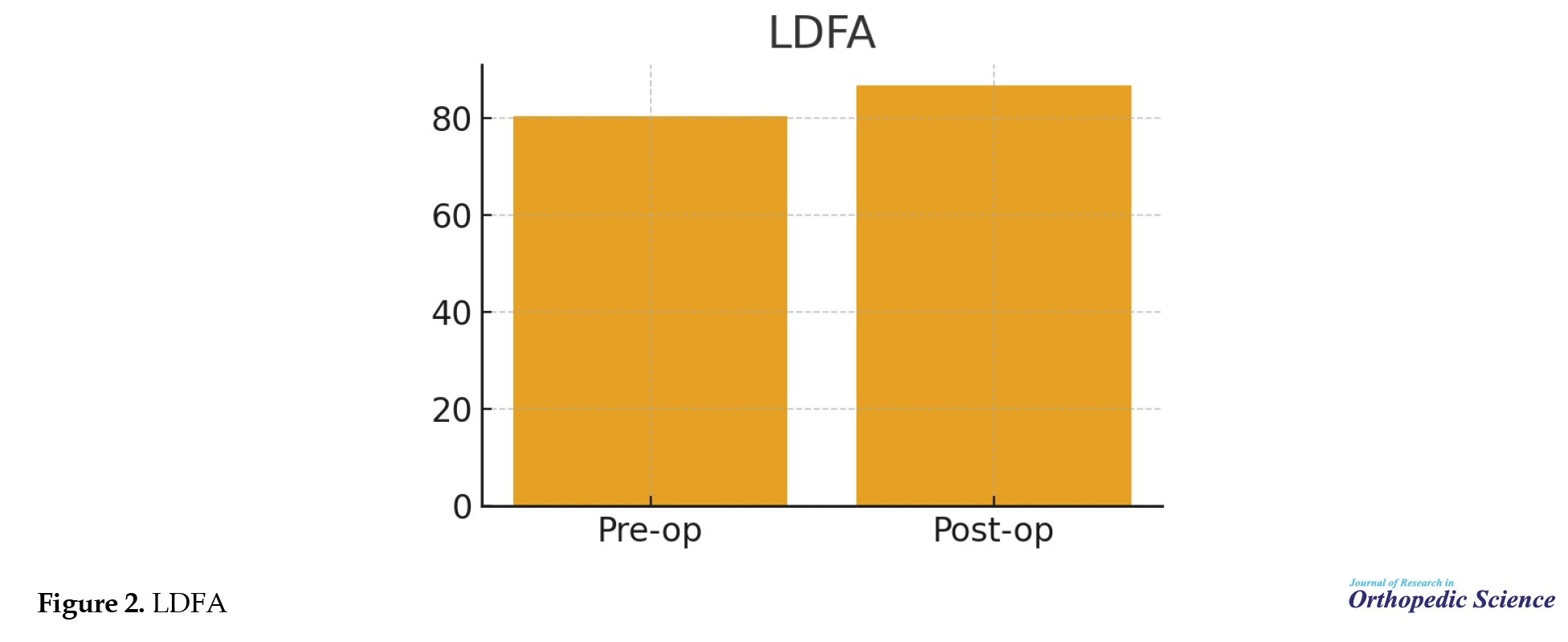
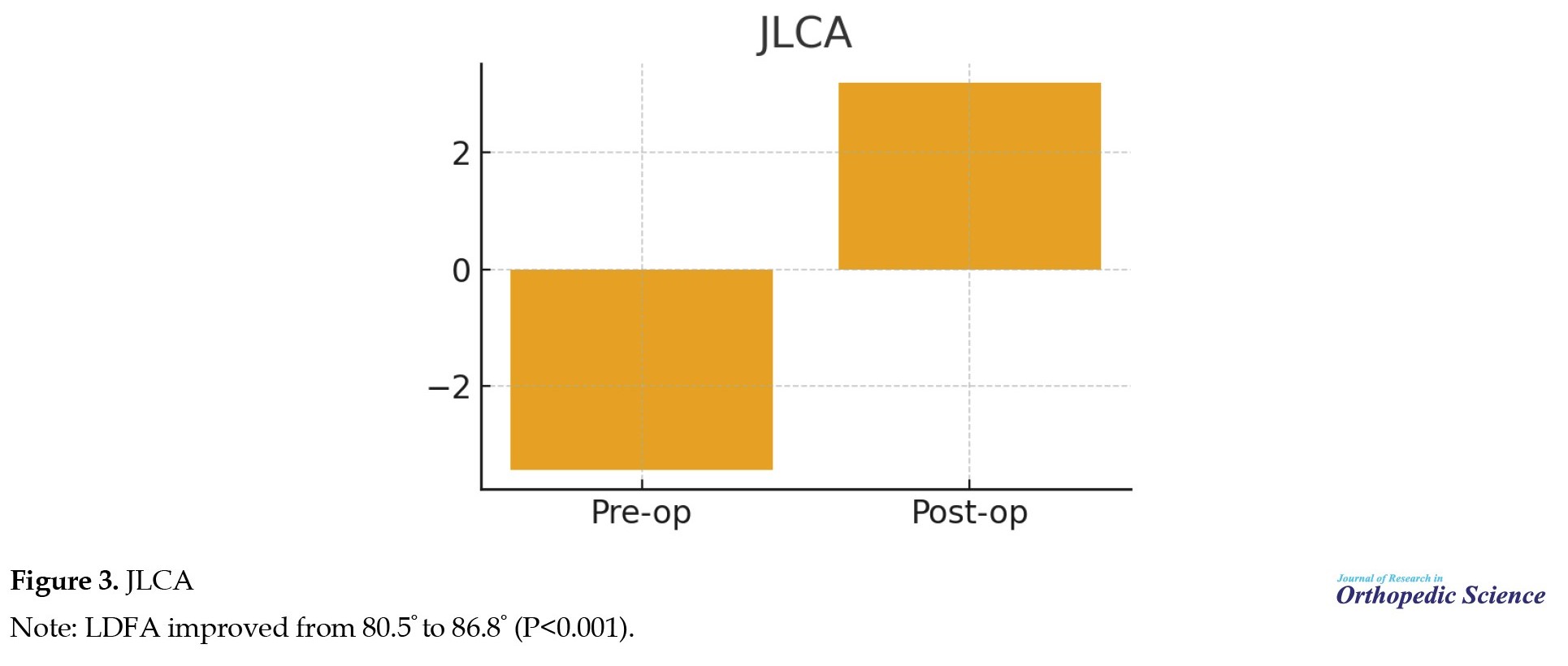
 LDFA increased from 80.5° to 86.8° (P<0.001). JLCA improved from −3.44° to 3.2° (P<0.001). The mechanical valgus angle decreased from 14° to 6.5° (P<0.001). MPTA changed from 90.4° to 89.8° and this difference was not statistically significant (P=0.10). Radiographic outcomes are presented in Table 3 and Figures 2, 3, 4 and 5.
LDFA increased from 80.5° to 86.8° (P<0.001). JLCA improved from −3.44° to 3.2° (P<0.001). The mechanical valgus angle decreased from 14° to 6.5° (P<0.001). MPTA changed from 90.4° to 89.8° and this difference was not statistically significant (P=0.10). Radiographic outcomes are presented in Table 3 and Figures 2, 3, 4 and 5.

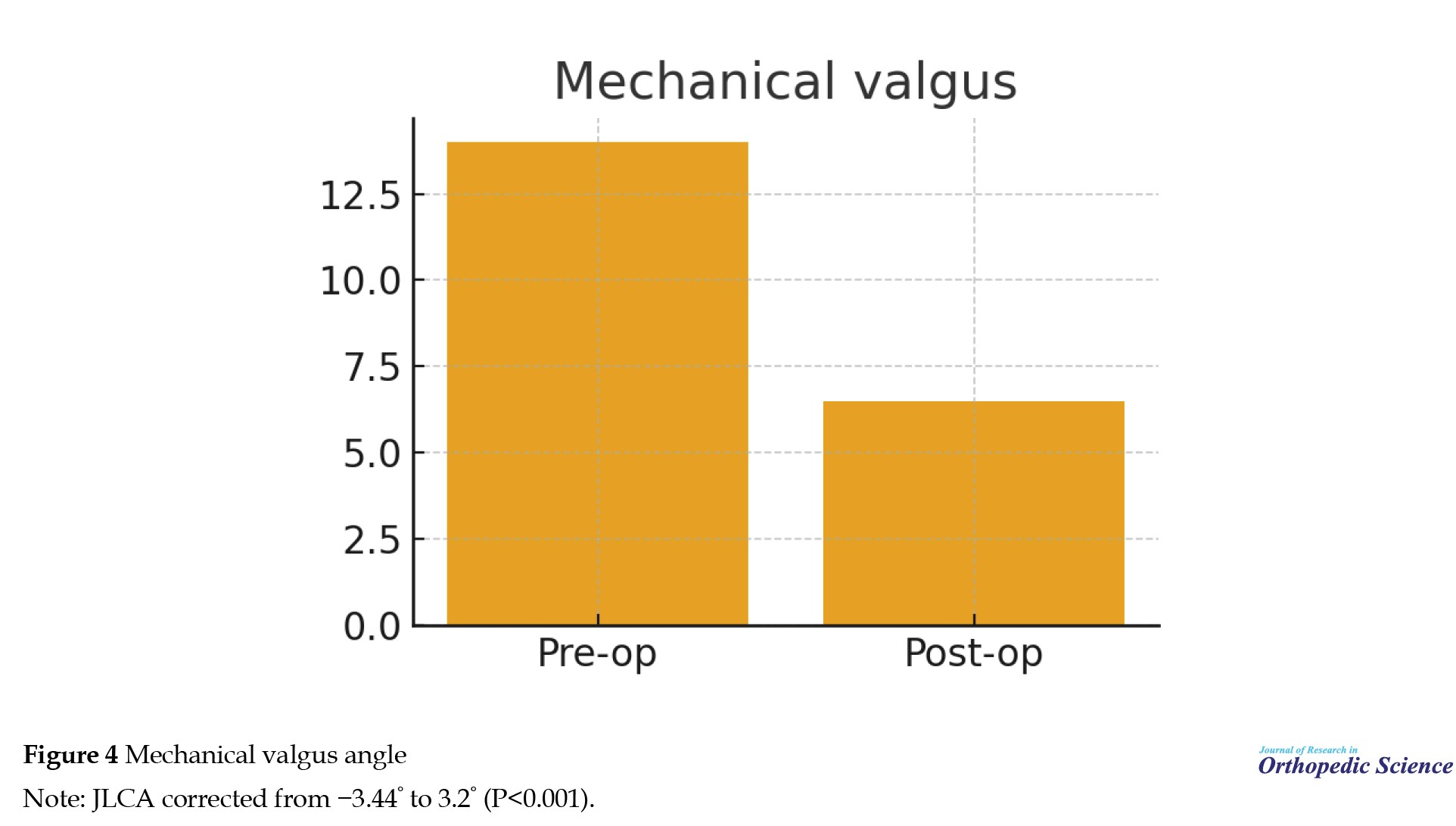
 MPTA showed no significant change (P=0.10). Mean knee ROM decreased from 127.9° preoperatively to 121.8° at final follow-up. No patient required further intervention for stiffness. Mean KOOS at final follow-up was 79.6 (range 66–99), and mean WOMAC was 23.5 (range 17–29), indicating satisfactory mid-term functional outcomes (Figures 6, 7, and 8).
MPTA showed no significant change (P=0.10). Mean knee ROM decreased from 127.9° preoperatively to 121.8° at final follow-up. No patient required further intervention for stiffness. Mean KOOS at final follow-up was 79.6 (range 66–99), and mean WOMAC was 23.5 (range 17–29), indicating satisfactory mid-term functional outcomes (Figures 6, 7, and 8).

 Final WOMAC scores (mean 23.5, range 17–29) reflect acceptable symptom levels. Seven knees (20.6%) underwent elective plate removal due to hardware irritation after :union:. One non:union: (2.9%) occurred and required revision. No cases of loss of correction, progressive joint-line obliquity, or recurrent valgus deformity were observed.
Final WOMAC scores (mean 23.5, range 17–29) reflect acceptable symptom levels. Seven knees (20.6%) underwent elective plate removal due to hardware irritation after :union:. One non:union: (2.9%) occurred and required revision. No cases of loss of correction, progressive joint-line obliquity, or recurrent valgus deformity were observed.
Discussion
The principal finding of this study is that assigning osteotomy to the anatomical source of valgus deformity resulted in reliable coronal correction and preservation of joint-line orientation. Most deformities in this cohort were femoral-based, in agreement with previous work that identified the distal femur as the dominant contributor in many adult valgus knees [4-8]. In such cases, DFO remains an appropriate and effective solution. The presence of tibial-based and combined deformities, however, confirms that valgus malalignment is not uniformly femoral and highlights the need for systematic radiographic analysis rather than a one-size-fits-all approach [3, 9-11].
The changes observed in LDFA, JLCA, and overall valgus angle are comparable to those reported in earlier DFO series using both closing- and opening-wedge techniques [4-8, 13-15]. Our data support the concept that matching the correction site to the origin of deformity improves joint-line orientation. In combined deformities, distributing correction through DLO avoids excessive wedge magnitude at a single site and helps maintain a horizontal joint line, in line with the rationale described by Backstein et al. [3] and Babis et al. [12].
Tibial-based deformity was uncommon in this cohort, but targeted PTO achieved acceptable alignment in these cases. Although the small number precludes detailed statistical analysis, the results align with established experience in valgus tibial osteotomy [16, 17] and emphasize that femur-only correction is not appropriate when the primary deviation lies in the tibia.
Functional outcomes in this series were satisfactory and comparable to prior reports of DFO in relatively young patients with valgus deformity [1, 7-9]. The modest reduction in flexion range did not translate into clinically relevant stiffness, and the rate of hardware-related symptoms requiring plate removal was consistent with other plate-fixed osteotomy series. The single non:union: observed was in line with reported non:union: rates for opening-wedge DFO [7, 8, 13-15].
This study has limitations. The retrospective design introduces potential selection bias, and the number of tibial-based and combined deformities was small, limiting subgroup analysis. Preoperative patient-reported outcome data were incomplete in some patients, which restricts analysis of change over time. The follow-up period, while adequate to confirm :union: and early stability of correction, did not allow conclusions about long-term survivorship or conversion to arthroplasty.
Despite these limitations, the findings support a practical, reproducible algorithm based on standardized long-leg radiographs. Identifying the anatomical origin of deformity and tailoring the correction accordingly appears to yield reliable alignment, preserves joint-line orientation, and produces functional outcomes that are consistent with established series.
Conclusion
In this cohort of adults with symptomatic valgus knee deformity, directing osteotomy to the anatomical source of malalignment produced reliable correction and preserved joint-line orientation. Most deformities were femoral-based and were effectively treated with DFO. Tibial-based and combined deformities were less common, but when present, proximal tibial or DLO restored alignment without inducing postoperative joint-line tilt. Functional outcomes were satisfactory, and serious complications were uncommon. Origin-specific planning based on standardized long-leg radiographs is a practical and reproducible strategy for valgus realignment in physiologically young adults.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of School of Medicine, Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.FMD.REC.1399.387).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Behnam Sour; Data collection: Bushra Zareie, Mohammadreza Heidarikhoo, and Behnam Sour; Data analysis: Bushra Zareie; Investigation: Abolfazl Bagherifard and Mahmoud Jabalameli; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Valgus malalignment alters coronal-plane mechanics by shifting the mechanical axis laterally, increasing load across the lateral tibiofemoral compartment. In physiologically young adults with persistent symptoms, realignment osteotomy remains a dependable joint-preserving option. Its effectiveness, however, depends on correcting the deformity at the anatomical level responsible for the deviation. When correction is performed at the wrong segment, the mechanical axis may be restored, but the joint line can remain oblique, creating abnormal shear forces and compromising load distribution [1-3].
Distal femoral varus osteotomy (DFO) has historically been the standard treatment for symptomatic valgus deformity. Closing-wedge and, more recently, lateral opening-wedge techniques have produced reliable correction, solid :union:, and durable pain relief in several series, particularly when deformity originates in the distal femur [4-8]. However, detailed long-leg radiographic analysis has shown that valgus deformity does not always arise from the femur alone. Some patients demonstrate proximal tibial involvement, and others exhibit combined femoral, tibial, and intra-articular contributions [3, 9-11]. In such cases, a femur-only osteotomy may normalize the mechanical axis yet leave the joint line tilted.
Objective radiographic measures—the lateral distal femoral angle (LDFA), medial proximal tibial angle (MPTA), and joint-line convergence angle (JLCA)—provide a structured framework for identifying the anatomical source of deformity [1-3]. An origin-directed approach assigns the osteotomy to the segment demonstrating the primary deviation and uses double-level correction when both segments contribute substantially or when JLCA suggests an intra-articular component [12]. Although widely acknowledged conceptually, few clinical series have applied this strategy as a systematic decision algorithm.
The purpose of the present study was to evaluate an origin-specific approach to valgus realignment in adults. Deformities were classified by their anatomical origin using standardized long-leg radiographs, and patients underwent distal femoral, proximal tibial, or Double-level osteotomy (DLO) accordingly. We aimed to determine whether this strategy yields accurate coronal correction, preserves joint-line orientation, and produces satisfactory mid-term clinical outcomes.
Methods
Study design and ethical approval
This retrospective study was conducted at a tertiary orthopedic referral center. All adult patients who underwent realignment surgery for symptomatic valgus knee deformity between 2011 and 2018 were screened. The study protocol was approved by the institutional review board, and all participants provided informed consent.
Patient selection
Inclusion criteria were symptomatic coronal-plane valgus deformity confirmed on standing long-leg radiographs, age appropriate for joint-preserving surgery, and a minimum of two years of radiographic and clinical follow-up. Indications included lateral compartment pain related to valgus overload, progressive deformity, post-traumatic malalignment, ligamentous insufficiency with valgus thrust, neuromuscular sequelae, or early osteoarthritis in physiologically young adults.
Exclusion criteria were previous realignment surgery around the knee, metabolic bone disease, incomplete imaging, or inability to complete follow-up. Thirty-one patients (34 knees) met the criteria and were included.
Radiographic assessment
Standardized standing long-leg anteroposterior radiographs were obtained with the patella directed forward and both hips and ankles included. Imaging was performed under full weight-bearing. Measurements were performed digitally on PACS by the operating surgeon or a senior fellow.
Three parameters were assessed: LDFA, defined as the angle between the femoral mechanical axis and distal femoral joint line; MPTA, defined as the angle between the tibial mechanical axis and proximal tibial joint line; and JLCA, defined as the angle between the distal femoral and proximal tibial joint lines. Normal reference values (LDFA ≈ 87°, MPTA ≈ 87°, JLCA ≈ 0–2°) were used to determine deformity origin [1-3].
Classification of deformity origin
Deformities were classified as femoral-based, tibial-based, or combined deformities. This algorithm guided the selection of DFO, PTO, or DLO [1-3, 12].
Surgical techniques
Distal femoral osteotomy (DFO) was used for femoral-based deformity, typically employing a lateral opening-wedge technique. Through a lateral approach, the distal femur was exposed and a biplanar osteotomy created under fluoroscopic guidance, preserving a medial cortical hinge. The wedge was opened to the planned correction and fixed with a locking compression plate [4-8, 13-15].
Proximal tibial osteotomy (PTO) was used for tibial-based deformity. A medial approach was used to perform a medial opening- or closing-wedge osteotomy according to anatomy and surgeon preference, with careful preservation of posterior tibial slope [16, 17]. Fixation was achieved with a locking plate.
DLO was used for combined deformity or markedly increased JLCA. The correction magnitude was divided between distal femur and proximal tibia to maintain joint-line orientation while restoring the mechanical axis [3, 12].
Postoperative management
Passive and active-assisted motion began on the first postoperative day. The goal was to reach at least 90° of flexion by four weeks and a functional range of motion (ROM) by six weeks. Partial weight-bearing was initiated after early callus formation, typically at eight weeks, and progressed to full weight-bearing by ten to twelve weeks based on radiographic :union: and clinical tolerance.
Outcome measures
Radiographic outcomes included LDFA, MPTA, JLCA, and mechanical valgus angle, recorded preoperatively and at final follow-up. Clinical outcomes included knee ROM, Western Ontario and McMaster universities osteoarthritis index (WOMAC), and knee injury and osteoarthritis outcome score (KOOS). Validated Persian versions of WOMAC and KOOS were used when applicable [18-20]. Complications, such as non:union:, hardware irritation requiring removal, loss of correction, and recurrent valgus were recorded.
Statistical analysis
Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Preoperative and final follow-up values were compared using paired t-tests when normally distributed and non-parametric tests when appropriate. Categorical variables were compared using chi-square tests. Statistical significance was set at P<0.05.
Results
Thirty-one patients (34 knees) met the inclusion criteria. The cohort included 26 women (83.9%) and 5 men (16.1%), with a mean age of 34.8±9.9 years and a mean body mass index (BMI) of 23.3±2.9 kg/m². Mean follow-up duration was 4.2±2.7 years. Laterality was evenly distributed (14 right, 14 left), and three patients (9.6%) had bilateral procedures. Indications included valgus overload pain, progressive deformity, post-traumatic malalignment, ligamentous insufficiency with valgus thrust, neuromuscular conditions, and early osteoarthritis. Baseline characteristics are summarized in Table 1.
Radiographically, 26 knees (76.5%) showed femoral-based deformity, 2 knees (5.9%) had tibial-based deformity, and 6 knees (17.6%) had combined deformity or marked JLCA. The distribution of deformity origin is shown in Table 2 and Figure 1.
Discussion
The principal finding of this study is that assigning osteotomy to the anatomical source of valgus deformity resulted in reliable coronal correction and preservation of joint-line orientation. Most deformities in this cohort were femoral-based, in agreement with previous work that identified the distal femur as the dominant contributor in many adult valgus knees [4-8]. In such cases, DFO remains an appropriate and effective solution. The presence of tibial-based and combined deformities, however, confirms that valgus malalignment is not uniformly femoral and highlights the need for systematic radiographic analysis rather than a one-size-fits-all approach [3, 9-11].
The changes observed in LDFA, JLCA, and overall valgus angle are comparable to those reported in earlier DFO series using both closing- and opening-wedge techniques [4-8, 13-15]. Our data support the concept that matching the correction site to the origin of deformity improves joint-line orientation. In combined deformities, distributing correction through DLO avoids excessive wedge magnitude at a single site and helps maintain a horizontal joint line, in line with the rationale described by Backstein et al. [3] and Babis et al. [12].
Tibial-based deformity was uncommon in this cohort, but targeted PTO achieved acceptable alignment in these cases. Although the small number precludes detailed statistical analysis, the results align with established experience in valgus tibial osteotomy [16, 17] and emphasize that femur-only correction is not appropriate when the primary deviation lies in the tibia.
Functional outcomes in this series were satisfactory and comparable to prior reports of DFO in relatively young patients with valgus deformity [1, 7-9]. The modest reduction in flexion range did not translate into clinically relevant stiffness, and the rate of hardware-related symptoms requiring plate removal was consistent with other plate-fixed osteotomy series. The single non:union: observed was in line with reported non:union: rates for opening-wedge DFO [7, 8, 13-15].
This study has limitations. The retrospective design introduces potential selection bias, and the number of tibial-based and combined deformities was small, limiting subgroup analysis. Preoperative patient-reported outcome data were incomplete in some patients, which restricts analysis of change over time. The follow-up period, while adequate to confirm :union: and early stability of correction, did not allow conclusions about long-term survivorship or conversion to arthroplasty.
Despite these limitations, the findings support a practical, reproducible algorithm based on standardized long-leg radiographs. Identifying the anatomical origin of deformity and tailoring the correction accordingly appears to yield reliable alignment, preserves joint-line orientation, and produces functional outcomes that are consistent with established series.
Conclusion
In this cohort of adults with symptomatic valgus knee deformity, directing osteotomy to the anatomical source of malalignment produced reliable correction and preserved joint-line orientation. Most deformities were femoral-based and were effectively treated with DFO. Tibial-based and combined deformities were less common, but when present, proximal tibial or DLO restored alignment without inducing postoperative joint-line tilt. Functional outcomes were satisfactory, and serious complications were uncommon. Origin-specific planning based on standardized long-leg radiographs is a practical and reproducible strategy for valgus realignment in physiologically young adults.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of School of Medicine, Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.FMD.REC.1399.387).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Behnam Sour; Data collection: Bushra Zareie, Mohammadreza Heidarikhoo, and Behnam Sour; Data analysis: Bushra Zareie; Investigation: Abolfazl Bagherifard and Mahmoud Jabalameli; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Smith J, Wilson A, Thomas N. Osteotomy around the knee: Evolution, principles and results. Knee Surg Sports Traumatol Arthrosc. 2013; 21(1):3-22. [DOI:10.1007/s00167-012-2206-0] [PMID]
- Puddu G, Cipolla M, Cerullo G, Franco V, Giannì E. Which osteotomy for a valgus knee? Int Orthop. 2010; 34(2):239-47. [DOI:10.1007/s00264-009-0820-3] [PMID]
- Backstein D, Morag G, Hanna S, Safir O, Gross A. Long-term follow-up of distal femoral varus osteotomy of the knee. J Arthroplasty. 2007; 22(4 Suppl 1):2-6. [DOI:10.1016/j.arth.2007.01.026] [PMID]
- McDermott AG, Finklestein JA, Farine IT, Boynton EL, MacIntosh DL, Gross A. Distal femoral varus osteotomy for valgus deformity of the knee. J Bone Joint Surg. 1988; 70(1):110-6. [DOI:10.2106/00004623-198870010-00017]
- Finkelstein JA, Gross AE, Davis A. Varus osteotomy of the distal part of the femur. A survivorship analysis. JBJS. 1996; 78(9):1348-52. [DOI:10.2106/00004623-199609000-00008] [PMID]
- Wang JW, Hsu CC. Distal femoral varus osteotomy for osteoarthritis of the knee. JBJS. 2005; 87(1):127-33. [DOI:10.2106/JBJS.C.01559]
- Kosashvili Y, Safir O, Gross A, Morag G, Lakstein D, Backstein D. Distal femoral varus osteotomy for lateral osteoarthritis of the knee: A minimum ten-year follow-up. Int Orthop. 2010; 34(2):249-54. [DOI:10.1007/s00264-009-0807-0] [PMID]
- Jabalameli M, Bagheri Fard A, Jahansouz A, Mokhtari T. Distal femoral varus osteotomy in 27 young patients with genu valgum. Tehran Univ Med J. 2014; 71(11):713. [Link]
- Haviv B, Bronak S, Thein R, Thein R. The results of corrective osteotomy for valgus arthritic knees. Knee Surg Sports Traumatol Arthrosc. 2013; 21(1):49-56. [DOI:10.1007/s00167-012-2180-6] [PMID]
- Saragaglia D, Chedal-Bornu B. Computer-assisted osteotomy for valgus knees: Medium-term results of 29 cases. Orthop Traumatol Surg Res. 2014; 100(5):527-30. [DOI:10.1016/j.otsr.2014.04.002] [PMID]
- Jacobi M, Wahl P, Bouaicha S, Jakob RP, Gautier E. Distal femoral varus osteotomy: Problems associated with the lateral open-wedge technique. Arch Orthop Trauma Surg. 2011; 131(6):725-8. [DOI:10.1007/s00402-010-1193-1] [PMID]
- Babis GC, An KN, Chao EY, Rand JA, Sim FH. Double level osteotomy of the knee: a method to retain joint-line obliquity. Clinical results. J Bone Joint Surg Am. 2002; 84(8):1380-8. [DOI:10.2106/00004623-200208000-00013] [PMID]
- O'Malley MP, Pareek A, Reardon PJ, Stuart MJ, Krych AJ. Distal femoral osteotomy: Lateral opening wedge technique. Arthrosc Tech. 2016; 5(4):e725-30. [DOI:10.1016/j.eats.2016.02.037] [PMID]
- Mitchell JJ, Dean CS, Chahla J, Moatshe G, Cram TR, LaPrade RF. Varus-producing lateral distal femoral opening-wedge osteotomy. Arthrosc Tech. 2016; 5(4):e799-e807. [DOI:10.1016/j.eats.2016.03.009] [PMID]
- Wylie JD, Maak TG. Medial closing-wedge distal femoral osteotomy for genu valgum with lateral compartment disease. Arthrosc Tech. 2016; 5(6):e1357-66. [DOI:10.1016/j.eats.2016.08.009] [PMID]
- Coventry M. Proximal tibial varus osteotomy for osteoarthritis of the lateral compartment of the knee. JBJS. 1987; 69(1):32-8. [DOI:10.2106/00004623-198769010-00006]
- Eberbach H, Mehl J, Feucht MJ, Bode G, Südkamp NP, Niemeyer P. Geometry of the valgus knee: Contradicting the dogma of a femoral-based deformity. Am J Sports Med. 2017; 45(4):909-14. [DOI:10.1177/0363546516676266] [PMID]
- Nadrian H, Moghimi N, Nadrian E, Moradzadeh R, Bahmanpour K, Iranpour A, et al. Validity and reliability of the Persian versions of WOMAC osteoarthritis index and lequesne algofunctional index. Clin Rheumatol. 2012; 31(7):1097-102. [DOI:10.1007/s10067-012-1983-7] [PMID]
- Ebrahimzadeh MH, Makhmalbaf H, Birjandinejad A, Keshtan FG, Hoseini HA, Mazloumi SM. The Western Ontario and McMaster universities osteoarthritis index (WOMAC) in Persian speaking patients with knee osteoarthritis. Arch Bone Jt Surg. 2014; 2(1):57-62. [PMID]
- Salavati M, Mazaheri M, Negahban H, Sohani SM, Ebrahimian MR, Ebrahimi I, et al. Validation of a Persian-version of knee injury and osteoarthritis outcome score (KOOS) in Iranians with knee injuries. Osteoarthritis Cartilage. 2008; 16(10):1178-82. [DOI:10.1016/j.joca.2008.03.004] [PMID]
Type of Study: Research Article |
Subject:
Knee surgery
Received: 2025/03/1 | Accepted: 2025/05/22 | Published: 2025/08/1
Received: 2025/03/1 | Accepted: 2025/05/22 | Published: 2025/08/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
