

Volume 12, Issue 4 (Autumn 2025)
JROS 2025, 12(4): 181-186 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nakahei Amroodi M, Tabrizian P, Mahdavifar M, Bahaeddini M, Anaraki Mohammadi M, Hashemipour B et al . Clinical Outcomes of Total Physeal Separation in Pediatric Distal Humerus Fractures: A Single-center Experience. JROS 2025; 12 (4) :181-186
URL: http://jros.iums.ac.ir/article-1-2308-en.html
URL: http://jros.iums.ac.ir/article-1-2308-en.html
Morteza Nakahei Amroodi1 

 , Pouria Tabrizian1 , Mohammadmehdi Mahdavifar1 , Mohammadreza Bahaeddini1 , Masoud Anaraki Mohammadi1 , Babak Hashemipour1 , Mojtaba Khajeh Alizadeh Attar1
, Pouria Tabrizian1 , Mohammadmehdi Mahdavifar1 , Mohammadreza Bahaeddini1 , Masoud Anaraki Mohammadi1 , Babak Hashemipour1 , Mojtaba Khajeh Alizadeh Attar1
, Pouria Tabrizian1 , Mohammadmehdi Mahdavifar1 , Mohammadreza Bahaeddini1 , Masoud Anaraki Mohammadi1 , Babak Hashemipour1 , Mojtaba Khajeh Alizadeh Attar1
1- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Total physeal separation (TPS), Distal humerus, Pediatric, Closed reduction, Percutaneous pinning, Elbow range of motion (ROM)
Full-Text [PDF 555 kb]
(37 Downloads)
| Abstract (HTML) (166 Views)
Full-Text: (10 Views)
Introduction
Distal humerus physeal separation (DHPS) is an uncommon injury that occurs predominantly in infants and young children. Because the distal humeral ossification centers are not fully developed in this age group, conventional radiographs often fail to clearly demonstrate the physis, leading to frequent misdiagnosis as supracondylar fractures or soft-tissue injury. Early case series have shown that DHPS may be initially overlooked in up to half of presenting cases, resulting in delays in appropriate management [1, 2].
The overall incidence of DHPS is lower than that of other pediatric elbow injuries, and most evidence on its natural history and optimal treatment is derived from case reports and small case series. However, a recent systematic review of the literature encompassing over 250 children with DHPS found that the mean age of affected patients was <18 months, and non-accidental trauma contributed substantially to the injury in infants [2].
The diagnosis of this injury remains challenging because the classic ossification centers of the distal humerus (such as the capitellum and trochlea) appear sequentially over several years, making assessment based on plain radiographs difficult in very young patients. This diagnostic uncertainty often necessitates supplemental imaging such as ultrasonography or magnetic resonance imaging (MRI) to confirm physeal disruption [3].
Management options for DHPS vary depending on the degree of displacement and patient age. While nondisplaced injuries may be treated with immobilization alone, displaced physeal separations are most commonly addressed with reduction maneuvers. Closed reduction and percutaneous pinning (CRPP) are frequently preferred and have been shown to provide stable fixation with satisfactory functional outcomes. In contrast, simple casting may be associated with higher rates of malalignment and subsequent deformity [2].
Long-term outcomes following CRPP have generally been favorable, with low incidences of significant complications such as cubitus varus and avascular necrosis when compared with conservative treatment alone. Arthrogram-assisted closed pinning has also been described as a useful technique to enhance anatomic reduction and minimize post-traumatic deformities [4].
Despite these encouraging results, the rarity of DHPS and the heterogeneity of available reports highlight the need for additional clinical studies with systematic follow-up to better characterize functional outcomes and complication profiles in contemporary practice.
Methods
This retrospective study included all children under 12 years diagnosed with total physeal separation (TPS) of the distal humerus and treated at Shafayahyaeian Hospital between 2011 and 2023. TPS is a rare pediatric elbow injury, often misdiagnosed as a more common fracture, such as a supracondylar fracture. All patients with a confirmed diagnosis based on clinical examination and radiographic findings were considered eligible.
The inclusion criteria included age 0–12 years, confirmed TPS diagnosis, availability of at least one pre-treatment imaging study, treatment with CRPP, and at least one post-treatment evaluation including range of motion (ROM), neurovascular status, and complications. The exclusion criteria included alternative treatments (e.g. open reduction and internal fixation [ORIF] or cast alone), incomplete records, or severe concomitant injuries that could confound outcomes.
Patient records were extracted from the hospital information system and reviewed individually to confirm TPS. The data collected included demographics, mechanism of injury, initial clinical findings, treatment details, and post-treatment outcomes, such as ROM, nerve function, and complications. Imaging studies—including plain radiographs and, in some infants, ultrasound—were reviewed to assess displacement, anatomical alignment, and pin position. After data collection, patient information was entered into SPSS software, version 26.
Given the rarity of this injury, the final sample consisted of all eligible patients over the 12-year period, using a total enumeration approach similar to that used in retrospective pediatric studies. Data were recorded using a standardized extraction form to ensure consistency. All procedures were approved by the Institutional Ethics Committee.
Results
A total of 13 patients with TPS of the distal humerus treated with CRPP at Shafayahyaeian Hospital between 2011 and 2023 were included in this study. The results are presented descriptively in the text and summarized in Tables 1, 2, 3, 4, 5, 6, and 7, covering demographic characteristics, mechanism of injury, neurovascular status, elbow ROM, and post-treatment complications.
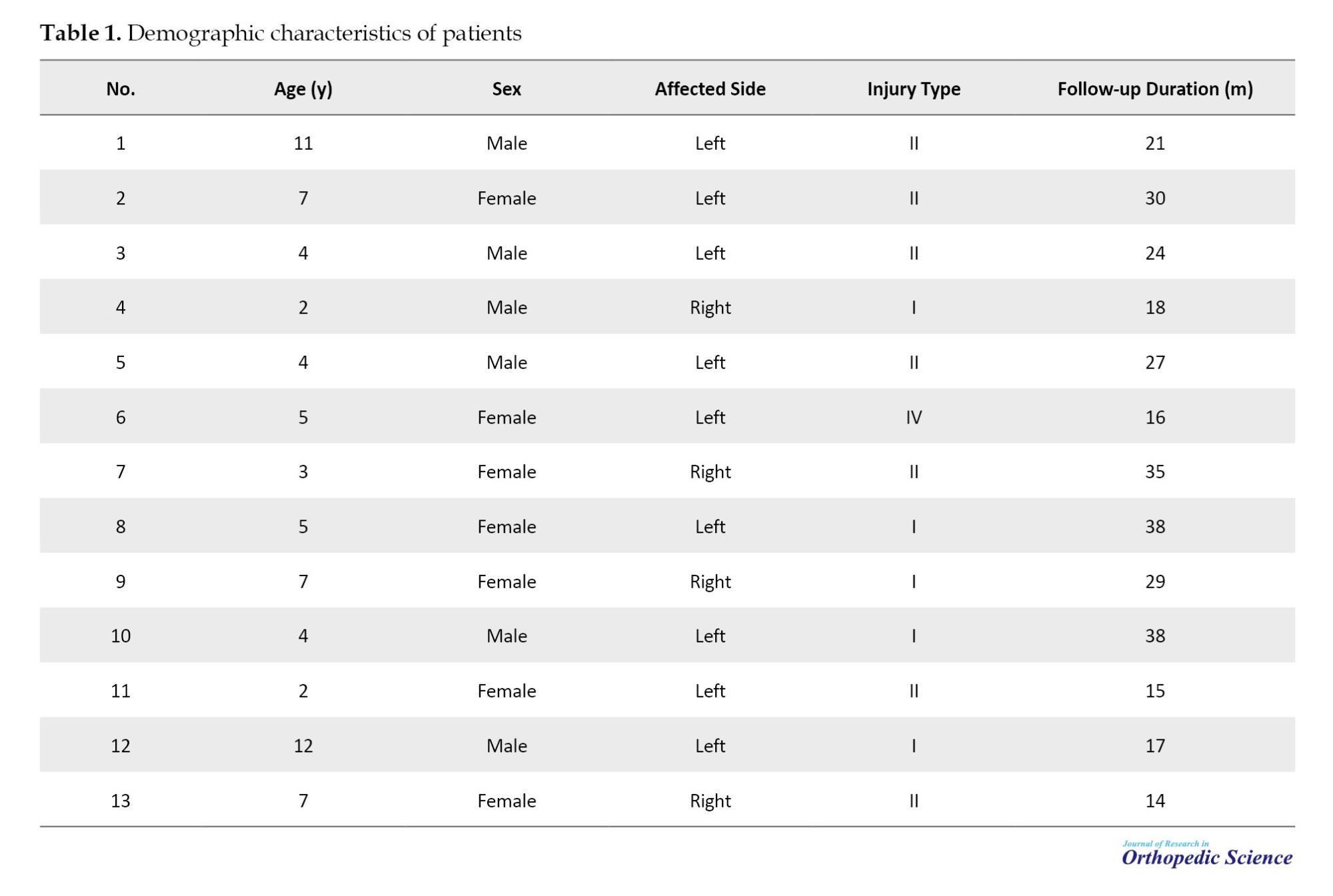
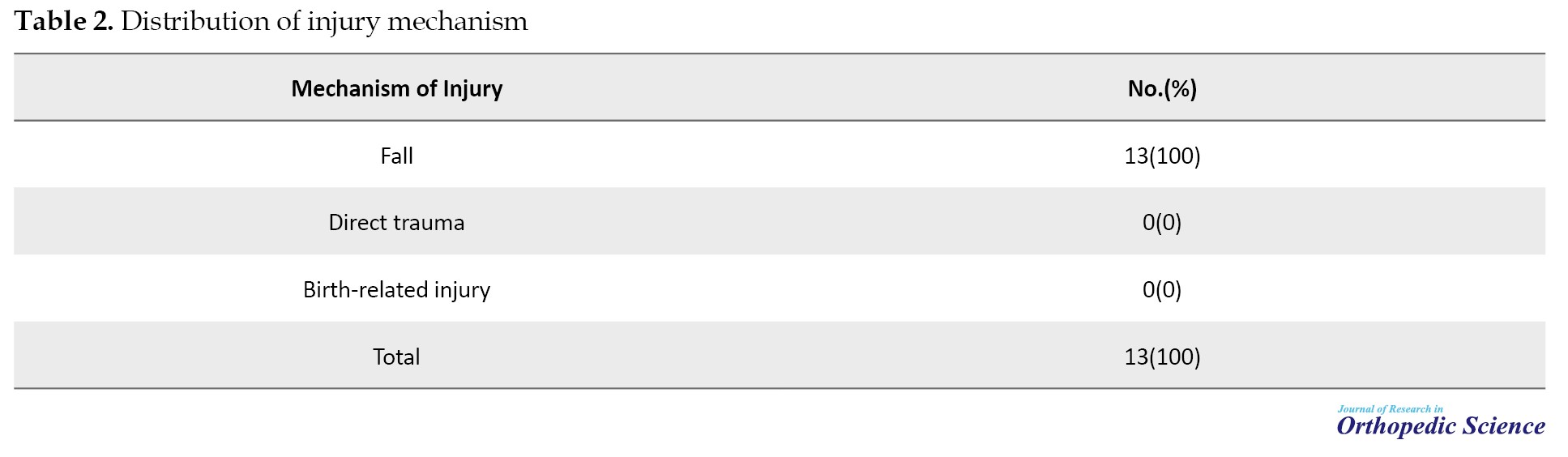
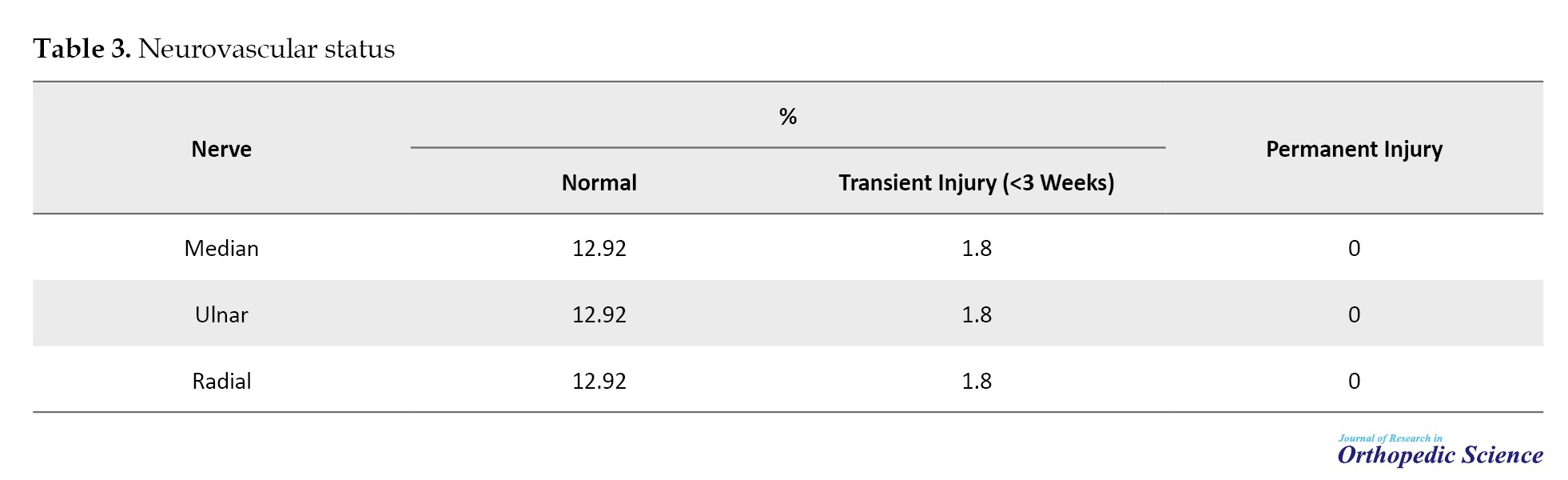
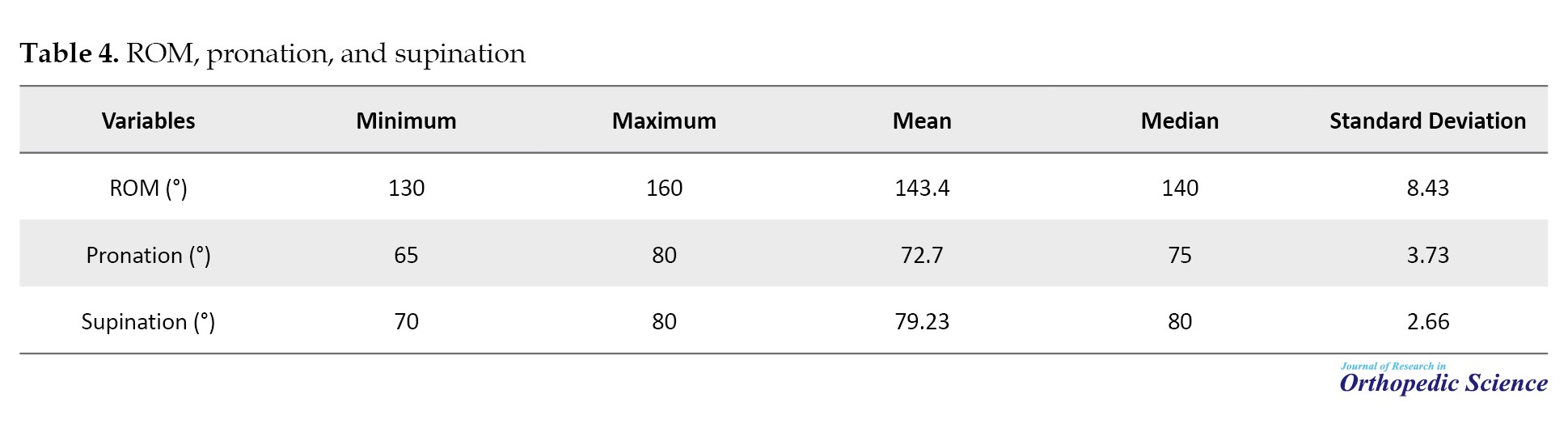
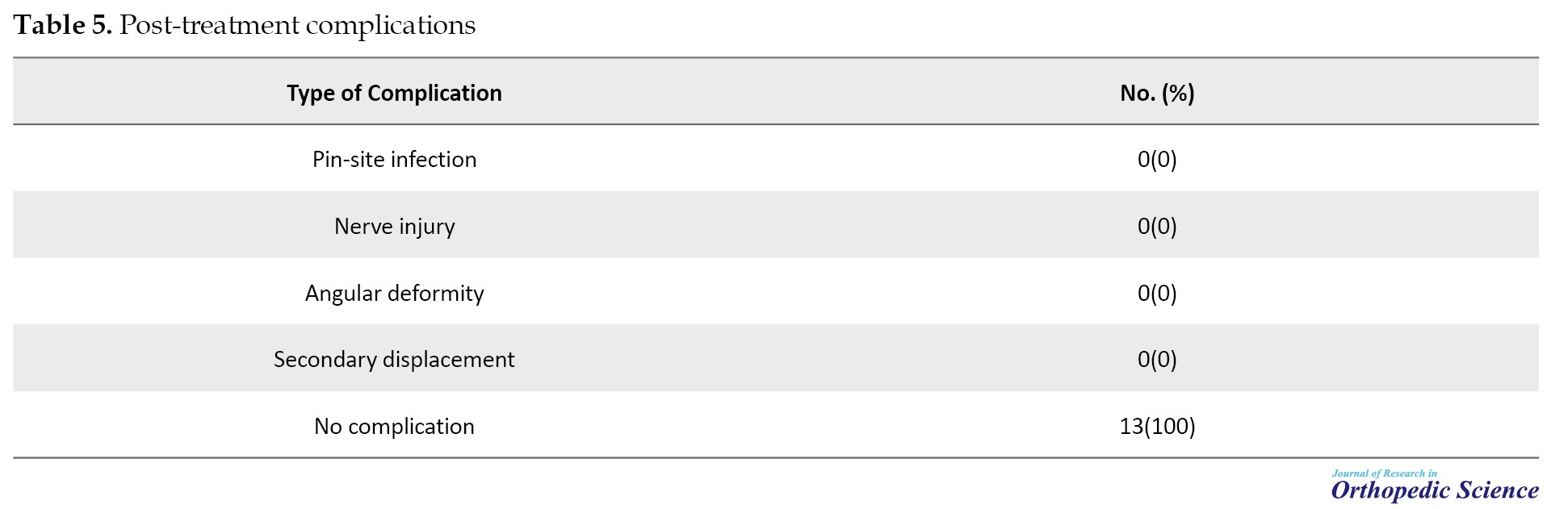
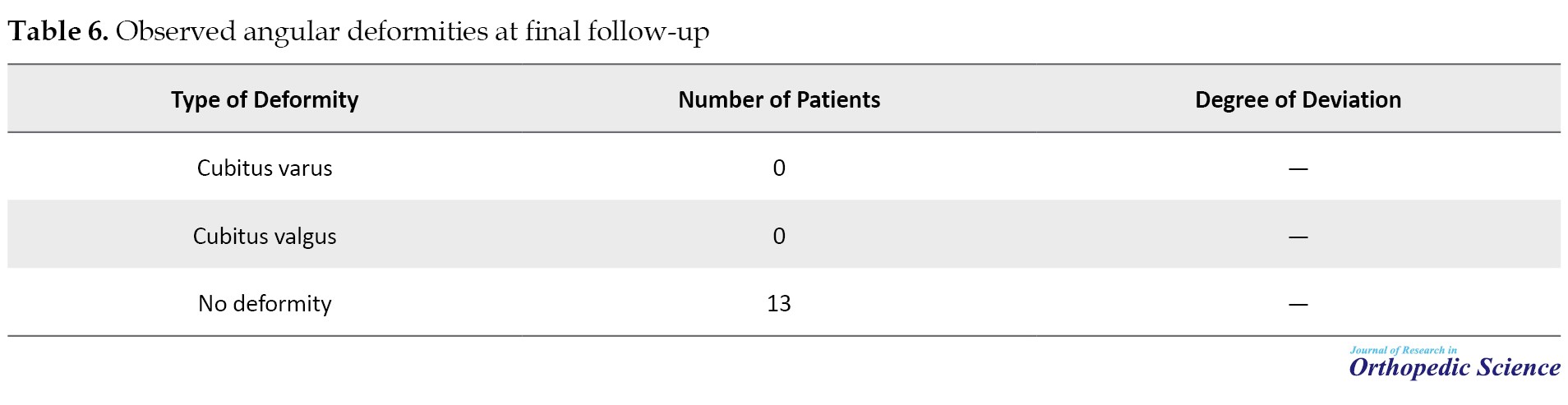
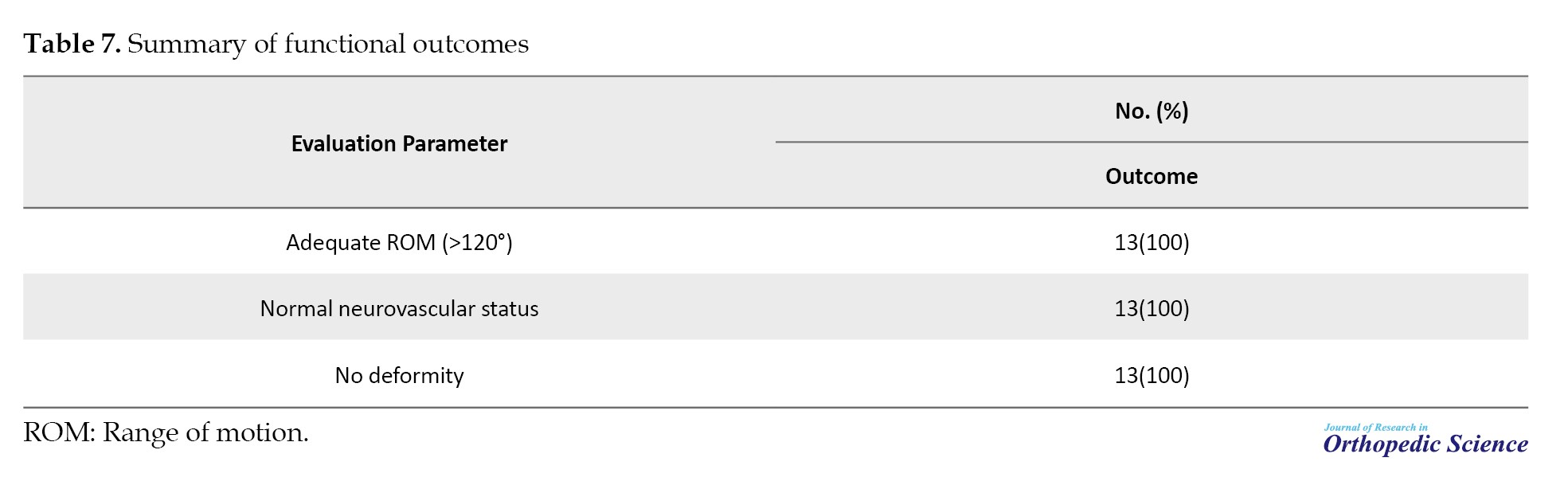
As shown in Table 1, the patients’ ages ranged from 2 to 12 years, and both sexes were represented. Injuries involved both the left and right upper limbs. The type of injury recorded in all cases corresponded to complete distal humeral physeal separation. The duration of follow-up varied among patients, with a minimum of one post-treatment visit documented for all, allowing assessment of functional and neurovascular outcomes. According to Table 2, the mechanism of injury in all patients was reported as fall, with no cases of direct trauma or birth-related injury. This finding is consistent with previous reports indicating falls as the most common cause of distal humeral physeal injuries in children. Post-treatment neurovascular evaluations indicated that all patients had normal nerve function (Table 3). Three patients experienced transient nerve injuries—ulnar, anterior interosseous, and posterior interosseous nerves—that resolved completely within three weeks. No permanent nerve deficits were observed, suggesting that CRPP effectively preserves the neurovascular structures around the elbow. Table 4 presents the final elbow ROM measurements. All patients achieved functional ROM, with most reaching near-normal flexion and extension. No patient demonstrated severe movement restriction, indicating satisfactory recovery of joint function following CRPP and follow-up. As summarized in Table 5, no major complications—including pin-site infection, persistent nerve injury, secondary displacement, or clinically significant deformity—were reported. All patients were classified in the “no complication” category, reflecting the safety and effectiveness of CRPP in this cohort. Follow-up evaluations revealed no cases of cubitus varus or cubitus valgus (Table 6). The absence of angular deformities indicates maintenance of proper anatomical alignment and satisfactory limb growth after treatment. Table 7 summarizes overall functional outcomes. All patients (100%) demonstrated appropriate ROM, normal neurovascular status, and no deformities. These results indicate that CRPP for distal humeral physeal separation provides excellent functional recovery in children.
Discussion
Studies on DHPS in children indicate that, despite its relatively low incidence, this injury presents significant diagnostic and therapeutic challenges, with initial misdiagnosis or delayed recognition reported in many cases. The existing body of evidence—particularly classical and authoritative studies in pediatric orthopedics—emphasizes the importance of accurate radiographic assessment, appropriate therapeutic intervention, and long-term follow-up.
In a foundational study, DeLee et al. classified patients into three age groups and reported that the clinical and radiographic features of DHPS vary according to skeletal maturity, highlighting the difficulty of early diagnosis in very young children [5]. Similarly, Gilbert and Conklin, in a cohort of 101 children under three years of age, demonstrated that only seven patients had true physeal separation, and none were correctly diagnosed on initial evaluation by emergency physicians or radiologists [1]. This finding underscores the high risk of misdiagnosis associated with this type of injury.
In recent decades, supplementary imaging modalities have gained attention. Supakul et al. demonstrated the utility of ultrasonography in confirming suspected cases, particularly in infants and young children in whom radiographs are limited by the largely cartilaginous structure of the elbow [6]. Akbarnia et al. highlighted the role of arthrography in infants with an unossified capitellum [7].
Other studies in children under three years old have reported that this age group exhibits the highest incidence of DHPS, often associated with falls. These studies also emphasize the importance of comparing the radius axis with the capitellum for accurate diagnosis [8]. Additionally, Jacobsen et al. showed that closed reduction in neonates yields excellent outcomes, with the high regenerative potential of the immature bone playing a crucial role in recovery [9].
Regarding treatment, most studies agree that CRPP is the standard of care for children older than six months with significant displacement [9, 10]. Open reduction is generally reserved for cases in which repeated attempts at closed reduction fail or interposed soft tissue prevents anatomic alignment [11]. Conversely, reports, such as Mathew et al. indicate that open reduction, particularly when not strictly necessary, may increase the risk of physeal injury or neurovascular complications and should therefore be approached cautiously [12].
The long-term functional outcomes reported in the literature generally indicate acceptable restoration of ROM and a low incidence of permanent nerve injury. For example, Sferopoulos observed that most patients achieved nearly normal ROM after appropriate treatment, with only a small proportion experiencing residual limitations [13]. Case reports by Mane and Challawar further stress that delayed diagnosis can lead to persistent angular deformities and poor functional results [14].
Conclusion
Based on this study’s findings, CRPP appears to be a safe and effective treatment for total distal humeral physeal separation in children, with favorable functional outcomes. In the patient cohort evaluated, CRPP was associated with preservation of neurovascular integrity, satisfactory restoration of elbow ROM, absence of angular deformities, and no major post-treatment complications. These results suggest that with accurate diagnosis and timely intervention, CRPP can achieve excellent therapeutic outcomes while minimizing the risk of long-term sequelae in pediatric patients with this rare injury.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.FMD.REC.1403.534).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Distal humerus physeal separation (DHPS) is an uncommon injury that occurs predominantly in infants and young children. Because the distal humeral ossification centers are not fully developed in this age group, conventional radiographs often fail to clearly demonstrate the physis, leading to frequent misdiagnosis as supracondylar fractures or soft-tissue injury. Early case series have shown that DHPS may be initially overlooked in up to half of presenting cases, resulting in delays in appropriate management [1, 2].
The overall incidence of DHPS is lower than that of other pediatric elbow injuries, and most evidence on its natural history and optimal treatment is derived from case reports and small case series. However, a recent systematic review of the literature encompassing over 250 children with DHPS found that the mean age of affected patients was <18 months, and non-accidental trauma contributed substantially to the injury in infants [2].
The diagnosis of this injury remains challenging because the classic ossification centers of the distal humerus (such as the capitellum and trochlea) appear sequentially over several years, making assessment based on plain radiographs difficult in very young patients. This diagnostic uncertainty often necessitates supplemental imaging such as ultrasonography or magnetic resonance imaging (MRI) to confirm physeal disruption [3].
Management options for DHPS vary depending on the degree of displacement and patient age. While nondisplaced injuries may be treated with immobilization alone, displaced physeal separations are most commonly addressed with reduction maneuvers. Closed reduction and percutaneous pinning (CRPP) are frequently preferred and have been shown to provide stable fixation with satisfactory functional outcomes. In contrast, simple casting may be associated with higher rates of malalignment and subsequent deformity [2].
Long-term outcomes following CRPP have generally been favorable, with low incidences of significant complications such as cubitus varus and avascular necrosis when compared with conservative treatment alone. Arthrogram-assisted closed pinning has also been described as a useful technique to enhance anatomic reduction and minimize post-traumatic deformities [4].
Despite these encouraging results, the rarity of DHPS and the heterogeneity of available reports highlight the need for additional clinical studies with systematic follow-up to better characterize functional outcomes and complication profiles in contemporary practice.
Methods
This retrospective study included all children under 12 years diagnosed with total physeal separation (TPS) of the distal humerus and treated at Shafayahyaeian Hospital between 2011 and 2023. TPS is a rare pediatric elbow injury, often misdiagnosed as a more common fracture, such as a supracondylar fracture. All patients with a confirmed diagnosis based on clinical examination and radiographic findings were considered eligible.
The inclusion criteria included age 0–12 years, confirmed TPS diagnosis, availability of at least one pre-treatment imaging study, treatment with CRPP, and at least one post-treatment evaluation including range of motion (ROM), neurovascular status, and complications. The exclusion criteria included alternative treatments (e.g. open reduction and internal fixation [ORIF] or cast alone), incomplete records, or severe concomitant injuries that could confound outcomes.
Patient records were extracted from the hospital information system and reviewed individually to confirm TPS. The data collected included demographics, mechanism of injury, initial clinical findings, treatment details, and post-treatment outcomes, such as ROM, nerve function, and complications. Imaging studies—including plain radiographs and, in some infants, ultrasound—were reviewed to assess displacement, anatomical alignment, and pin position. After data collection, patient information was entered into SPSS software, version 26.
Given the rarity of this injury, the final sample consisted of all eligible patients over the 12-year period, using a total enumeration approach similar to that used in retrospective pediatric studies. Data were recorded using a standardized extraction form to ensure consistency. All procedures were approved by the Institutional Ethics Committee.
Results
A total of 13 patients with TPS of the distal humerus treated with CRPP at Shafayahyaeian Hospital between 2011 and 2023 were included in this study. The results are presented descriptively in the text and summarized in Tables 1, 2, 3, 4, 5, 6, and 7, covering demographic characteristics, mechanism of injury, neurovascular status, elbow ROM, and post-treatment complications.
As shown in Table 1, the patients’ ages ranged from 2 to 12 years, and both sexes were represented. Injuries involved both the left and right upper limbs. The type of injury recorded in all cases corresponded to complete distal humeral physeal separation. The duration of follow-up varied among patients, with a minimum of one post-treatment visit documented for all, allowing assessment of functional and neurovascular outcomes. According to Table 2, the mechanism of injury in all patients was reported as fall, with no cases of direct trauma or birth-related injury. This finding is consistent with previous reports indicating falls as the most common cause of distal humeral physeal injuries in children. Post-treatment neurovascular evaluations indicated that all patients had normal nerve function (Table 3). Three patients experienced transient nerve injuries—ulnar, anterior interosseous, and posterior interosseous nerves—that resolved completely within three weeks. No permanent nerve deficits were observed, suggesting that CRPP effectively preserves the neurovascular structures around the elbow. Table 4 presents the final elbow ROM measurements. All patients achieved functional ROM, with most reaching near-normal flexion and extension. No patient demonstrated severe movement restriction, indicating satisfactory recovery of joint function following CRPP and follow-up. As summarized in Table 5, no major complications—including pin-site infection, persistent nerve injury, secondary displacement, or clinically significant deformity—were reported. All patients were classified in the “no complication” category, reflecting the safety and effectiveness of CRPP in this cohort. Follow-up evaluations revealed no cases of cubitus varus or cubitus valgus (Table 6). The absence of angular deformities indicates maintenance of proper anatomical alignment and satisfactory limb growth after treatment. Table 7 summarizes overall functional outcomes. All patients (100%) demonstrated appropriate ROM, normal neurovascular status, and no deformities. These results indicate that CRPP for distal humeral physeal separation provides excellent functional recovery in children.
Discussion
Studies on DHPS in children indicate that, despite its relatively low incidence, this injury presents significant diagnostic and therapeutic challenges, with initial misdiagnosis or delayed recognition reported in many cases. The existing body of evidence—particularly classical and authoritative studies in pediatric orthopedics—emphasizes the importance of accurate radiographic assessment, appropriate therapeutic intervention, and long-term follow-up.
In a foundational study, DeLee et al. classified patients into three age groups and reported that the clinical and radiographic features of DHPS vary according to skeletal maturity, highlighting the difficulty of early diagnosis in very young children [5]. Similarly, Gilbert and Conklin, in a cohort of 101 children under three years of age, demonstrated that only seven patients had true physeal separation, and none were correctly diagnosed on initial evaluation by emergency physicians or radiologists [1]. This finding underscores the high risk of misdiagnosis associated with this type of injury.
In recent decades, supplementary imaging modalities have gained attention. Supakul et al. demonstrated the utility of ultrasonography in confirming suspected cases, particularly in infants and young children in whom radiographs are limited by the largely cartilaginous structure of the elbow [6]. Akbarnia et al. highlighted the role of arthrography in infants with an unossified capitellum [7].
Other studies in children under three years old have reported that this age group exhibits the highest incidence of DHPS, often associated with falls. These studies also emphasize the importance of comparing the radius axis with the capitellum for accurate diagnosis [8]. Additionally, Jacobsen et al. showed that closed reduction in neonates yields excellent outcomes, with the high regenerative potential of the immature bone playing a crucial role in recovery [9].
Regarding treatment, most studies agree that CRPP is the standard of care for children older than six months with significant displacement [9, 10]. Open reduction is generally reserved for cases in which repeated attempts at closed reduction fail or interposed soft tissue prevents anatomic alignment [11]. Conversely, reports, such as Mathew et al. indicate that open reduction, particularly when not strictly necessary, may increase the risk of physeal injury or neurovascular complications and should therefore be approached cautiously [12].
The long-term functional outcomes reported in the literature generally indicate acceptable restoration of ROM and a low incidence of permanent nerve injury. For example, Sferopoulos observed that most patients achieved nearly normal ROM after appropriate treatment, with only a small proportion experiencing residual limitations [13]. Case reports by Mane and Challawar further stress that delayed diagnosis can lead to persistent angular deformities and poor functional results [14].
Conclusion
Based on this study’s findings, CRPP appears to be a safe and effective treatment for total distal humeral physeal separation in children, with favorable functional outcomes. In the patient cohort evaluated, CRPP was associated with preservation of neurovascular integrity, satisfactory restoration of elbow ROM, absence of angular deformities, and no major post-treatment complications. These results suggest that with accurate diagnosis and timely intervention, CRPP can achieve excellent therapeutic outcomes while minimizing the risk of long-term sequelae in pediatric patients with this rare injury.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.FMD.REC.1403.534).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
- Gilbert SR, Conklin MJ. Presentation of distal humerus physeal separation. Pediatr Emerg Care. 2007; 23(11):816-9. [DOI:10.1097/PEC.0b013e31815a060b] [PMID]
- Chalidis B, Rigkos D, Giouleka S, Pitsilos C. Comparative outcomes of treatment strategies for traumatic distal humerus physeal separation in children: A systematic review. J Clin Med. 2025; 14(6):2037. [DOI:10.3390/jcm14062037] [PMID]
- Cheong WL, Kamisan N, Ismail II. Distal humerus physeal separation: Diagnostic challenges and implications. Cureus. 2024; 16(12). [DOI:10.7759/cureus.76248]
- Cha SM, Shin HD, Choi ES. Long-term outcomes of distal humeral epiphyseal separations treated via closed reduction and pinning under arthrogram. Injury. 2020; 51(2):207-11. [DOI:10.1016/j.injury.2019.11.038] [PMID]
- DeLee J, Wilkins KE, Rogers L, Rockwood C. Fracture-separation of the distal humeral epiphysis. JBJS. 1980; 62(1):46-51. [DOI:10.2106/00004623-198062010-00007]
- Supakul N, Hicks RA, Caltoum CB, Karmazyn B. Distal humeral epiphyseal separation in young children: an often-missed fracture-radiographic signs and ultrasound confirmatory diagnosis. Am J Roentgenol. 2015; 204(2):W192-W8. [DOI:10.2214/AJR.14.12788] [PMID]
- Akbarnia BA, Silberstein M, Rende R, Graviss E, Luisiri A. Arthrography in the diagnosis of fractures of the distal end of the humerus in infants. JBJS. 1986; 68(4):599-602. [DOI:10.2106/00004623-198668040-00018]
- Oh CW, Park BC, Ihn JC, Kyung HS. Fracture separation of the distal humeral epiphysis in children younger than three years old. J Pediatr Orthop. 2000; 20(2):173-6. [DOI:10.1097/00004694-200003000-00008]
- Jacobsen S, Hansson G, Nathorst-Westfelt J. Traumatic separation of the distal epiphysis of the humerus sustained at birth. J Bone Joint Surg Br Vol. 2009; 91(6):797-802. [DOI:10.1302/0301-620X.91B6.22140] [PMID]
- Rockwood CA. Rockwood and Wilkins’ fractures in children. Philadelphia: Lippincott Williams & Wilkins; 2010. [Link]
- De Jager L, Hoffman E. Fracture-separation of the distal humeral epiphysis. Bone Joint Surg Br Vol. 1991; 73(1):143-6. [DOI:10.1302/0301-620X.73B1.1991750] [PMID]
- Mathew DK, Gangadharan S, Krishnamoorthy V, Shanmughanathan R. Anterior physeal separation of distal humerus: Report of a rare case with review of literature. Indian J Orthop. 2021; 55(1):208-12. [DOI:10.1007/s43465-020-00111-9] [PMID]
- Sferopoulos NK, Anagnostopoulos D. Anterior dislocation of the elbow in a child with congenital posterior dislocation of the radial head. A case report. Acta Orthop Belg. 1999; 65(3):378-81. [PMID]
- Mane PP, Challawar NS, Shah H. Late presented case of distal humerus epiphyseal separation in a newborn. BMJ Case Rep. 2016; 2016:bcr2016215296. [DOI:10.1136/bcr-2016-215296] [PMID]
Type of Study: Research Article |
Subject:
Shoulder / Elbow
Received: 2025/02/12 | Accepted: 2025/06/16 | Published: 2025/11/1
Received: 2025/02/12 | Accepted: 2025/06/16 | Published: 2025/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
