

Volume 7, Issue 1 (2-2020)
JROS 2020, 7(1): 41-46 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nakhaee Amroodi M, Bagherifard A, Jabalameli M, Salehpour M, Majdi S. Alkaptonuric Ochronosis Superimposed With Septic Arthritis in a Middle-aged Man. JROS 2020; 7 (1) :41-46
URL: http://jros.iums.ac.ir/article-1-2055-en.html
URL: http://jros.iums.ac.ir/article-1-2055-en.html
Morteza Nakhaee Amroodi1 

 , Abolfazl Bagherifard1 , Mahmoud Jabalameli1 , Mostafa Salehpour1 , Shoeib Majdi1
, Abolfazl Bagherifard1 , Mahmoud Jabalameli1 , Mostafa Salehpour1 , Shoeib Majdi1
, Abolfazl Bagherifard1 , Mahmoud Jabalameli1 , Mostafa Salehpour1 , Shoeib Majdi1
1- Bone and Joint Reconstruction Research Center, Shafa Orthopedic Hospital, Iran University of Medical Sciences,Tehran, Iran.
Full-Text [PDF 1093 kb]
(924 Downloads)



Full-Text: (977 Views)
1. Introduction
A lkaptonuria (AKU) is a rare autosomal recessive metabolic disease introduced in 1902 [1]. This disorder is associated with a deficiency in homogentisate 1,2-dioxygenase (homogentisic acid oxidase: HGO enzyme) and its activity in the liver. More than 100 mutated genes have been identified responsible for AKU on chromosome 3q13.33, encompassing 14 exons [2]. HGO splits the aromatic ring of Homogentisic Acid (HGA) (alkapton) at the third step of the phenylalanine metabolic pathway. The deficiency of HGO in patients with alkaptonuria causes the excretion of HGA in different body fluids, like urine. Darkening of urine is the only sign of the disorder in the pediatric age group, and it occurs at a very early stage of the disease. Oxidation and polymerization of the homogentisic acid is enhanced with alkaline pH. Therefore, acid urine may not darken after many hours of standing and this sign may not be seen in the patient. In such cases, the diagnosis may be delayed until adulthood, when other complications of the disease such as arthritis or ochronosis occur [3, 4].
Irreversibly polymerization and oxidation of HGA to benzoquinone acetic acid, produce melanin-like pigments in connective tissues. These pigments deposit in the skin, sclera, ear cartilage, genitalia, and nail beds, and accordingly damage vital organs of the body, including the cardiovascular and renal systems (aortic stenosis and nephrolithiasis) [5]. Nevertheless, more common symptoms of this disease that causes disability and impairs quality of life are the joint involvement [6], calcification and degeneration of synovial and intervertebral disks, and ossification of ligaments [7]. This gradual damage to the musculoskeletal system usually becomes symptomatic in the third or fourth decades of life, presenting as inflammatory arthritis in the acute phase or osteoarthritis in the chronic phase [8].
Since the enzymatic expression can be reduced by appropriate medications [9], misdiagnosis results in degenerative joint disease and joint replacement in many patients [4]. Therefore, presenting more cases can help increase physician’s knowledge about the symptoms and appropriate treatment of this rare disease.
In this study, we report a 49-year-old man presenting with knee swelling and pain, who ultimately diagnosed as alkaptonuria ochronosis and received the appropriate treatment.
2. Case Presentation
A 49-year-old man referred to the emergency department of Shafa Yahyaian Hospital in March 2018 with left knee pain, low-grade fever, and mild illness without a history of trauma. In his medical history, he had knee pain and swelling since 2 weeks ago. He also mentioned a mild hip pain. Thus, knee (Figure 1) and pelvic x-rays (Figure 2) were requested, which revealed mild Degenerative Joint Disease (DJD) in both knees and hips.
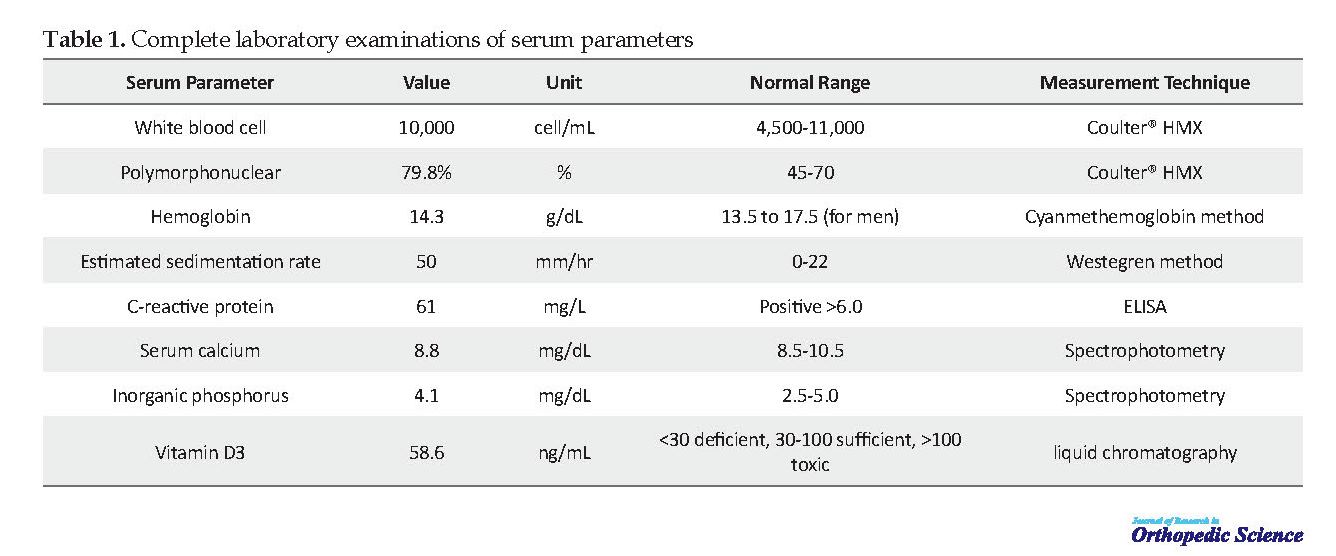
He was admitted to the Orthopedic Ward for further evaluation and treatment. In physical examination, he had pigmented sclera, as well as swelling, tenderness, and warmness in his left knee. Aspirated synovial fluid had turbid appearance and pale yellow color; White Blood Cell (WBC) of 80000 cells/ micro liter, Polymorphonuclear (PMN) cell of 90%, and Red Blood Cell (RBC) of 100 cells/ micro liter, first hour ESR was 50 mm/h, and CRP was 61 mg/L. Wright and Coombs tests were negative. Table 1 presents the results of complete laboratory examinations of serum parameters. On suspicion of septic arthritis, arthrotomy was done for the patient with a midline incision.
A lkaptonuria (AKU) is a rare autosomal recessive metabolic disease introduced in 1902 [1]. This disorder is associated with a deficiency in homogentisate 1,2-dioxygenase (homogentisic acid oxidase: HGO enzyme) and its activity in the liver. More than 100 mutated genes have been identified responsible for AKU on chromosome 3q13.33, encompassing 14 exons [2]. HGO splits the aromatic ring of Homogentisic Acid (HGA) (alkapton) at the third step of the phenylalanine metabolic pathway. The deficiency of HGO in patients with alkaptonuria causes the excretion of HGA in different body fluids, like urine. Darkening of urine is the only sign of the disorder in the pediatric age group, and it occurs at a very early stage of the disease. Oxidation and polymerization of the homogentisic acid is enhanced with alkaline pH. Therefore, acid urine may not darken after many hours of standing and this sign may not be seen in the patient. In such cases, the diagnosis may be delayed until adulthood, when other complications of the disease such as arthritis or ochronosis occur [3, 4].
Irreversibly polymerization and oxidation of HGA to benzoquinone acetic acid, produce melanin-like pigments in connective tissues. These pigments deposit in the skin, sclera, ear cartilage, genitalia, and nail beds, and accordingly damage vital organs of the body, including the cardiovascular and renal systems (aortic stenosis and nephrolithiasis) [5]. Nevertheless, more common symptoms of this disease that causes disability and impairs quality of life are the joint involvement [6], calcification and degeneration of synovial and intervertebral disks, and ossification of ligaments [7]. This gradual damage to the musculoskeletal system usually becomes symptomatic in the third or fourth decades of life, presenting as inflammatory arthritis in the acute phase or osteoarthritis in the chronic phase [8].
Since the enzymatic expression can be reduced by appropriate medications [9], misdiagnosis results in degenerative joint disease and joint replacement in many patients [4]. Therefore, presenting more cases can help increase physician’s knowledge about the symptoms and appropriate treatment of this rare disease.
In this study, we report a 49-year-old man presenting with knee swelling and pain, who ultimately diagnosed as alkaptonuria ochronosis and received the appropriate treatment.
2. Case Presentation
A 49-year-old man referred to the emergency department of Shafa Yahyaian Hospital in March 2018 with left knee pain, low-grade fever, and mild illness without a history of trauma. In his medical history, he had knee pain and swelling since 2 weeks ago. He also mentioned a mild hip pain. Thus, knee (Figure 1) and pelvic x-rays (Figure 2) were requested, which revealed mild Degenerative Joint Disease (DJD) in both knees and hips.
He was admitted to the Orthopedic Ward for further evaluation and treatment. In physical examination, he had pigmented sclera, as well as swelling, tenderness, and warmness in his left knee. Aspirated synovial fluid had turbid appearance and pale yellow color; White Blood Cell (WBC) of 80000 cells/ micro liter, Polymorphonuclear (PMN) cell of 90%, and Red Blood Cell (RBC) of 100 cells/ micro liter, first hour ESR was 50 mm/h, and CRP was 61 mg/L. Wright and Coombs tests were negative. Table 1 presents the results of complete laboratory examinations of serum parameters. On suspicion of septic arthritis, arthrotomy was done for the patient with a midline incision.
During the surgical procedure, we observed the black appearance of the knee, especially its cartilages (Figure 3), and became suspicious of ochronosis, so we took a sample (4×2×1 cm) for pathologic examination and some synovial fluid for culture. Antibiotic therapy was initiated for the patient (vancomycin 1 g BD and imipenem 500 mg QID) intravenously, and rheumatologic consultation was requested. The rheumatologic specialist required bone densitometry, urine analysis, and measurement of serum levels of alkaline phosphatase, calcium, phosphorus, and vitamin D. Table 1 presents the results. Bone densitometry revealed osteopenic status in the spine (T-score of -1.2 and Z-score of -0.8) and osteoporotic status in the femoral neck (T-score of -3.7 and Z-score of -3.0).
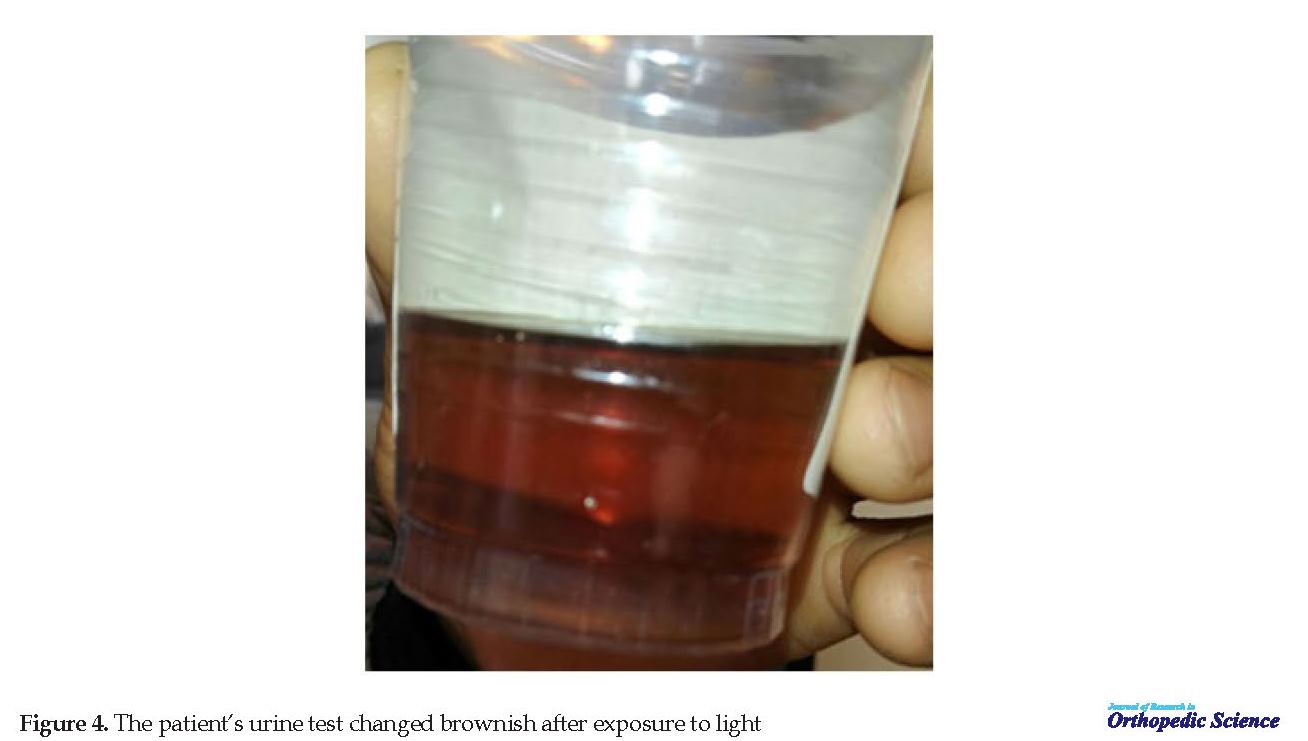
The patient’s urine test changed brownish after exposure to light (Figure 4) and confirmed the diagnosis. During the first week, waiting for the pathologic examination result, the patient’s status improved significantly. The ESR value decreased to 31 mm/h, while CRP was unchanged. The culture was negative after 48 hours and 14 days. The microscopic examination revealed black-brownish, sharply defined, irregular shaped and fragmented fibers in subintima. The pigment granules presented in endothelium and surface zones. Moderate infiltration of mixed inflammatory cells, predominantly PMN leukocytes, eosinophils, and plasma cells. Pathologic diagnosis was ochronosis superimposed by septic arthritis.
The patient’s urine test changed brownish after exposure to light (Figure 4) and confirmed the diagnosis. During the first week, waiting for the pathologic examination result, the patient’s status improved significantly. The ESR value decreased to 31 mm/h, while CRP was unchanged. The culture was negative after 48 hours and 14 days. The microscopic examination revealed black-brownish, sharply defined, irregular shaped and fragmented fibers in subintima. The pigment granules presented in endothelium and surface zones. Moderate infiltration of mixed inflammatory cells, predominantly PMN leukocytes, eosinophils, and plasma cells. Pathologic diagnosis was ochronosis superimposed by septic arthritis.
The following treatment was initiated for the patient, with final diagnosis of ochronosis: IV antibiotics were changed to ciprofloxacin tablet 500 mg BD and rifampin tablet 300 mg TDS, then 6 days later, Aclasta 5 mg one dose, and calcium + vitamin D tablets (contains 500 mg Ca and 200 mg vitamin D) to take every night. Antibiotic treatment was continued for one week.
3. Discussion
Alkaptonuria is a rare inborn metabolic disease, and the accumulation of HGA in tissues can gradually damage various systems, especially the musculoskeletal system [4]. Previous reports indicate that the disease may present as acute inflammatory arthritis or chronic osteoarthritis [8]. In our case, the patient had left knee swelling and pain for two weeks, and the initial diagnosis, based on physical examination and synovial aspiration, was septic arthritis, so he was treated with arthrotomy.
3. Discussion
Alkaptonuria is a rare inborn metabolic disease, and the accumulation of HGA in tissues can gradually damage various systems, especially the musculoskeletal system [4]. Previous reports indicate that the disease may present as acute inflammatory arthritis or chronic osteoarthritis [8]. In our case, the patient had left knee swelling and pain for two weeks, and the initial diagnosis, based on physical examination and synovial aspiration, was septic arthritis, so he was treated with arthrotomy.
Septic arthritis of the knee is the invasion of pathogenic organisms to the joint, commonly observed after trauma, which causes pain, swelling, and warmness [10]. Our patient had septic arthritis without any trauma but accompanied by alkaptonuric ochronosis. Most cases with alkaptonuric ochronosis report low back pain, kyphosis, scoliosis, and lumbar spine involvement; therefore, ankylosing spondylitis is considered one of the important differential diagnoses [11].
The chief complaint of our patient was acute knee pain, which is observed in 5 out of 7 patients, as reported by Azami et al. in Ardabil, but not as the chief complaint [12]. Knee pain has been reported as an accidental finding during a physical examination or imaging survey [13]. In a similar study, a 48-year-old male was reported with chronic knee pain (>2 years), which required total knee replacement due to advanced joint degeneration [14]. Fortunately, our patient referred with acute symptoms and mild DJD, while many cases remain undiagnosed until the fifth or sixth decade of their life with more pain and disability that necessitates joint replacement [11, 12]. Earlier diagnosis can prevent further degenerations and injuries. Although the joint replacement improves patient joint disorder, it increases the disease cost and burden [4].
The chief complaint of our patient was acute knee pain, which is observed in 5 out of 7 patients, as reported by Azami et al. in Ardabil, but not as the chief complaint [12]. Knee pain has been reported as an accidental finding during a physical examination or imaging survey [13]. In a similar study, a 48-year-old male was reported with chronic knee pain (>2 years), which required total knee replacement due to advanced joint degeneration [14]. Fortunately, our patient referred with acute symptoms and mild DJD, while many cases remain undiagnosed until the fifth or sixth decade of their life with more pain and disability that necessitates joint replacement [11, 12]. Earlier diagnosis can prevent further degenerations and injuries. Although the joint replacement improves patient joint disorder, it increases the disease cost and burden [4].
Alkaptonuric ochronosis can be diagnosed since birth with its apparent symptoms such as dark urine by standing, pigmentation in sclera, ear cartilage, and the skin [3]; however, patients and the family members may neither pay attention to these symptoms nor seek medical help so that the disease may remain undiagnosed until adulthood [4]. Besides, physicians may only look at the patient’s chief complaint and miss the rest of the symptoms that help correct diagnosis. The sooner the disease is diagnosed, the earlier the physician can prescribe medications (like nitisinone, which inhibits the enzyme-producing HGA [4-hydroxyphenylpyruvate dioxygenase]) [15] and help alleviate patients’ symptoms, although it may not serve as a cure [12]. In our case, we started vitamin D + calcium supplementation after the treatment of superimposed septic arthritis. Previously, Aliberti et al. reported the association of ochronosis with increased bone resorption leading to accelerated bone loss [16].
The disease incidence is as low as 1:1000000 in some countries, and it is generally a sporadic disease [17]. Although the exact prevalence is not known in Iran, very few cases have been reported so far [13]. Therefore, reporting any case can help physicians increase their knowledge about this disease, and its symptoms, in the patient and family members [3]. In this case, the patient remained undiagnosed until the age of 49 years. He had developed DJD in his joints, which was fortunately mild and did not require arthroplasty.
In conclusion, alkaptonuric ochronosis is a rare metabolic disease, and joint degeneration gradually occurs by the accumulation of HGA in connective tissues. Paying attention to all symptoms like pigmented skin, ear cartilage, and sclera, and urine oxidation (darkness) by standing can help diagnose the disease before the joint disorders cause disability and severe pain. Therefore, it is essential to report and study all cases worldwide to increase physicians’ awareness and knowledge about this rare disease.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Authors' contributions
Designing the study, reviewing-editing the manuscript and supervision: Morteza Nakhaei Amroodi, Abolfazl Bagherifard and Mahmoud Jabalameli1; Writing the manuscript: Morteza Nakhei Amroodi, Mostafa Salehpour; Data collection and analysis: Mostafa salehpour, Shoib majdi.
Conflict of interest
The authors declared no conflict of interest.
References
Garrod A. The incidence of alkaptonuria: A study in chemical individuality. Lancet. 1902; 160(4137):1616-20. [DOI:10.1016/S0140-6736(01)41972-6]
Rodríguez JM, Timm DE, Titus GP, Beltran-Valero De Bernabe D, Criado O, Mueller HA, et al. Structural and functional analysis of mutations in alkaptonuria. Hum Mol Genet. 2000; 9(15):2341-50. [DOI:10.1093/oxfordjournals.hmg.a018927] [PMID]
Peker E, Yonden Z, Sogut S. From darkening urine to early diagnosis of alkaptonuria. Indian J Dermatol Venereol Leprol. 2008; 74(6):700. [DOI:10.4103/0378-6323.45142] [PMID]
Phornphutkul C, Introne WJ, Perry MB, Bernardini I, Murphey MD, Fitzpatrick DL, et al. Natural history of alkaptonuria. N Engl J Med. 2002; 347(26):2111-21. [DOI:10.1056/NEJMoa021736] [PMID]
Fisher AA, Davis MW. Alkaptonuric ochronosis with aortic valve and joint replacements and femoral fracture: A case report and literature review. Clin Med Res. 2004; 2(4):209-15. [DOI:10.3121/cmr.2.4.209] [PMID] [PMCID]
Mistry JB, Bukhari M, Taylor AM. Alkaptonuria. Rare Dis. 2013; 1:e27475. [DOI:10.4161/rdis.27475] [PMID] [PMCID]
Keller JM, Macaulay W, Nercessian OA, Jaffe IA. New developments in ochronosis: review of the literature. Rheumatol Int. 2005; 25(2):81-5. [DOI:10.1007/s00296-004-0498-1] [PMID]
Zhao BH, Chen BC, Shao de C, Zhang Q. Osteoarthritis? Ochronotic arthritis! A case study and review of the literature. Knee Surg Sports Traumatol Arthrosc. 2009; 17(7):778-81. [DOI:10.1007/s00167-009-0778-0] [PMID]
Sykut-Cegielska J. Alkaptonuria--first inborn error of metabolism known for a century and new treatment option--preliminary report. Dev Period Med. 2015; 19(4):508-10.
Horowitz DL, Katzap E, Horowitz S, Barilla-LaBarca ML. Approach to septic arthritis. Am Fam Physician. 2011; 84(6):653-60. [PMID]
Perry MB, Suwannarat P, Furst GP, Gahl WA, Gerber LH. Musculoskeletal findings and disability in alkaptonuria. J Rheumatol. 2006; 33(11):2280-5. [PMID]
Azami A, Maleki N, Tavosi Z. Alkaptonuric ochronosis: a clinical study from Ardabil, Iran. Int J Rheum Dis. 2014; 17(3):327-32. [DOI:10.1111/1756-185X.12287] [PMID]
Zabihiyeganeh M, Chehrehgosha H, Mirzaei A. Undiagnosed ochronosis presented as severe osteoarthritis with concomitant osteoporotic fracture. Shafa Orthopedic Journal. 2016; 3(2):e4717. [DOI:10.17795/soj-4717]
Abimbola O, Hall G, Zuckerman JD. Degenerative arthritis of the knee secondary to ochronosis. Bull NYU Hosp Jt Dis. 2011; 69(4):331-4.
Suwannarat P, O’Brien K, Perry MB, Sebring N, Bernardini I, Kaiser-Kupfer MI, et al. Use of nitisinone in patients with alkaptonuria. Metab. 2005; 54(6):719-28. [DOI:10.1016/j.metabol.2004.12.017] [PMID]
Aliberti G, Pulignano I, Schiappoli A, Minisola S, Romagnoli E, Proietta M. Bone metabolism in ochronotic patients. J Intern Med. 2003; 254(3):296-300. [DOI:10.1046/j.1365-2796.2003.01145.x] [PMID]
Gürkanlar D, Daneyemez M, Solmaz I, Temiz C. Ochronosis and lumbar disc herniation. Acta Neurochir. 2006; 148(8):891-4. [DOI:10.1007/s00701-006-0774-9] [PMID]
In conclusion, alkaptonuric ochronosis is a rare metabolic disease, and joint degeneration gradually occurs by the accumulation of HGA in connective tissues. Paying attention to all symptoms like pigmented skin, ear cartilage, and sclera, and urine oxidation (darkness) by standing can help diagnose the disease before the joint disorders cause disability and severe pain. Therefore, it is essential to report and study all cases worldwide to increase physicians’ awareness and knowledge about this rare disease.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Authors' contributions
Designing the study, reviewing-editing the manuscript and supervision: Morteza Nakhaei Amroodi, Abolfazl Bagherifard and Mahmoud Jabalameli1; Writing the manuscript: Morteza Nakhei Amroodi, Mostafa Salehpour; Data collection and analysis: Mostafa salehpour, Shoib majdi.
Conflict of interest
The authors declared no conflict of interest.
References
Garrod A. The incidence of alkaptonuria: A study in chemical individuality. Lancet. 1902; 160(4137):1616-20. [DOI:10.1016/S0140-6736(01)41972-6]
Rodríguez JM, Timm DE, Titus GP, Beltran-Valero De Bernabe D, Criado O, Mueller HA, et al. Structural and functional analysis of mutations in alkaptonuria. Hum Mol Genet. 2000; 9(15):2341-50. [DOI:10.1093/oxfordjournals.hmg.a018927] [PMID]
Peker E, Yonden Z, Sogut S. From darkening urine to early diagnosis of alkaptonuria. Indian J Dermatol Venereol Leprol. 2008; 74(6):700. [DOI:10.4103/0378-6323.45142] [PMID]
Phornphutkul C, Introne WJ, Perry MB, Bernardini I, Murphey MD, Fitzpatrick DL, et al. Natural history of alkaptonuria. N Engl J Med. 2002; 347(26):2111-21. [DOI:10.1056/NEJMoa021736] [PMID]
Fisher AA, Davis MW. Alkaptonuric ochronosis with aortic valve and joint replacements and femoral fracture: A case report and literature review. Clin Med Res. 2004; 2(4):209-15. [DOI:10.3121/cmr.2.4.209] [PMID] [PMCID]
Mistry JB, Bukhari M, Taylor AM. Alkaptonuria. Rare Dis. 2013; 1:e27475. [DOI:10.4161/rdis.27475] [PMID] [PMCID]
Keller JM, Macaulay W, Nercessian OA, Jaffe IA. New developments in ochronosis: review of the literature. Rheumatol Int. 2005; 25(2):81-5. [DOI:10.1007/s00296-004-0498-1] [PMID]
Zhao BH, Chen BC, Shao de C, Zhang Q. Osteoarthritis? Ochronotic arthritis! A case study and review of the literature. Knee Surg Sports Traumatol Arthrosc. 2009; 17(7):778-81. [DOI:10.1007/s00167-009-0778-0] [PMID]
Sykut-Cegielska J. Alkaptonuria--first inborn error of metabolism known for a century and new treatment option--preliminary report. Dev Period Med. 2015; 19(4):508-10.
Horowitz DL, Katzap E, Horowitz S, Barilla-LaBarca ML. Approach to septic arthritis. Am Fam Physician. 2011; 84(6):653-60. [PMID]
Perry MB, Suwannarat P, Furst GP, Gahl WA, Gerber LH. Musculoskeletal findings and disability in alkaptonuria. J Rheumatol. 2006; 33(11):2280-5. [PMID]
Azami A, Maleki N, Tavosi Z. Alkaptonuric ochronosis: a clinical study from Ardabil, Iran. Int J Rheum Dis. 2014; 17(3):327-32. [DOI:10.1111/1756-185X.12287] [PMID]
Zabihiyeganeh M, Chehrehgosha H, Mirzaei A. Undiagnosed ochronosis presented as severe osteoarthritis with concomitant osteoporotic fracture. Shafa Orthopedic Journal. 2016; 3(2):e4717. [DOI:10.17795/soj-4717]
Abimbola O, Hall G, Zuckerman JD. Degenerative arthritis of the knee secondary to ochronosis. Bull NYU Hosp Jt Dis. 2011; 69(4):331-4.
Suwannarat P, O’Brien K, Perry MB, Sebring N, Bernardini I, Kaiser-Kupfer MI, et al. Use of nitisinone in patients with alkaptonuria. Metab. 2005; 54(6):719-28. [DOI:10.1016/j.metabol.2004.12.017] [PMID]
Aliberti G, Pulignano I, Schiappoli A, Minisola S, Romagnoli E, Proietta M. Bone metabolism in ochronotic patients. J Intern Med. 2003; 254(3):296-300. [DOI:10.1046/j.1365-2796.2003.01145.x] [PMID]
Gürkanlar D, Daneyemez M, Solmaz I, Temiz C. Ochronosis and lumbar disc herniation. Acta Neurochir. 2006; 148(8):891-4. [DOI:10.1007/s00701-006-0774-9] [PMID]
Type of Study: Research Article |
Subject:
Knee surgery
Received: 2019/07/5 | Accepted: 2019/12/10 | Published: 2020/02/1
Received: 2019/07/5 | Accepted: 2019/12/10 | Published: 2020/02/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
