

Volume 12, Issue 3 (Summer 2025)
JROS 2025, 12(3): 121-136 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ashoury H, Yalfani A. The Role of Water Kinetic Chain Exercises in Maximum Voluntary Isometric Contraction of Gluteus Medius and Quadratus Lumborum Muscles in Chronic Low Back Pain Patients: A Randomized Clinical Trial. JROS 2025; 12 (3) :121-136
URL: http://jros.iums.ac.ir/article-1-2297-en.html
URL: http://jros.iums.ac.ir/article-1-2297-en.html



1- Department of Physical Education and Sport Sciences, Payame Noor University, Tehran, Iran.
2- Department of Sport Rehabilitation, Faculty of Physical Education and Sport Sciences, Bu-Ali Sina University, Hamadan, Iran.
2- Department of Sport Rehabilitation, Faculty of Physical Education and Sport Sciences, Bu-Ali Sina University, Hamadan, Iran.
Keywords: Low back pain, Maximum voluntary isometric contraction (MVIC), Kinetic chain, Gluteus medius (GMed), Quadratus lumborum (QL)
Full-Text [PDF 1838 kb]
(121 Downloads)
| Abstract (HTML) (246 Views)
Full-Text: (54 Views)
Introduction
Chronic low back pain (CLBP) is a widespread condition that significantly impacts the lives of millions of individuals worldwide, often leading to physical limitations and diminished quality of life (QoL) [1-5]. It is characterized by persistent discomfort in the lower back that lasts for more than three months and can arise from various factors, including muscular imbalances, poor posture, and previous injuries [6-8]. The maximum voluntary isometric contraction (MVIC) is the peak force or torque a muscle group can generate in a single maximal effort against an immovable resistance [9-11]. It is a key measure in strength and conditioning, used to assess muscle function and track progress in training or rehabilitation [9, 12]. Studies suggest that weakened stabilizing muscles’ MVIC may contribute to instability and discomfort in individuals with CLBP [13-15]. Evaluating MVIC in the lumbar region helps identify deficits that may exacerbate CLBP and guide targeted rehabilitation strategies [12-15]. For instance, when larger and stronger muscles are activated first without proper assistance from smaller stabilizing muscles, this disparity may overload the lumbar structures and ultimately cause discomfort or pain [16]. Additionally, the regular application of an unsuitable activation sequence can lead to muscle fatigue, weakness, and a heightened injury risk, underscoring the necessity for correct movement mechanics and muscle coordination in averting CLBP [17]. Among the key contributors to CLBP are dysfunctions in the stabilizing muscles of the lumbar and pelvic regions, particularly the gluteus medius (GMed) and quadratus lumborum (QL) [18-20]. Impairments in the strength and coordination of these muscles can lead to altered biomechanics [21, 22], resulting in increased stress on the lumbar spine and contributing to the persistence of CLBP [23-28]. Their synergistic activation is essential for maintaining optimal pelvic alignment and spinal integrity during dynamic activities, thereby preventing compensatory movement patterns and reducing the risk of musculoskeletal injuries [22, 29]. Function coordination of these muscles is essential for maintaining pelvic stability and proper spinal alignment during movement [10, 24-26]. In general, adequate strengthening and coordination of the QL and GMed muscles can enhance muscular health and establish a stable base for the lower back, assisting in the prevention of CLBP [30].
Conventional rehabilitation methods typically emphasize the importance of strengthening essential muscles [19, 31]. However, numerous patients find it challenging to consistently engage in land-based exercise programs, often due to discomfort or concerns about worsening their condition [32-34]. Water-based exercise programs have emerged as a promising solution, leveraging the unique properties of water to create a supportive environment that reduces joint stress while providing resistance for muscle strengthening [6, 32, 35-42]. he human body should not be viewed as a collection of isolated muscles, bones, connective tissues, and ligaments; rather, it is an integrated system where each component influences the others, and this interaction can yield either beneficial or detrimental effects [43-50]. Ideally, when the motor chain is engaged, the body operates as a cohesive unit, facilitating smooth and efficient movements [50-54].
Water kinetic chain exercises (WKCe) utilize the buoyancy and resistance of water to facilitate movement patterns that mimic functional activities, allowing individuals to engage in exercises with reduced pain and increased range of motion [45, 47, 55- 58]. Despite the potential advantages of aquatic therapy, there remains a significant gap in the literature regarding its specific effects on muscle activation in patients with CLBP [59-62].
The lack of research underscores the necessity for systematic investigation into the efficacy of WKCe on performance. The present study aimed to explore the impact of WKCe on MVIC of the GMed and QL muscles in individuals suffering from chronic non-specific low back pain (CNSLBP). By comparing the outcomes of both intervention groups, this research sought to determine whether WKCe can provide superior benefits in enhancing muscle function and alleviating pain levels. The findings from this investigation could significantly inform clinical practice, encouraging the integration of aquatic exercise into treatment plans for CNSLBP. Ultimately, this research aspires to contribute to the growing body of evidence supporting innovative rehabilitation strategies, offering hope for improved recovery and enhanced QoL for individuals affected by CNSLBP. By addressing this significant health issue, the study aimed to pave the way for more effective, patient-centered rehabilitation approaches that meet the needs of those suffering from this debilitating condition.
Methods
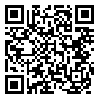
The present study employed a double-blind, randomized controlled pilot design to examine the effects of an intervention on individuals suffering from CNSLBP. To ensure reliable outcome assessments, comprehensive data collection was conducted both before and after the trial, incorporating subjective feedback and physiological evaluations [57]. Randomization was achieved by generating codes in blocks of four and six using Random Allocation Software, version 1.0 [63]. The allocation process was concealed with sequentially numbered, opaque, sealed envelopes, which were intentionally substantial to highlight their importance [64]. An orthopedic specialist diagnosed participants with CNSLBP following MRI scans and physical examinations. Sixty participants were randomly assigned to three groups of twenty to maintain balance within the study. One group served as the control, while another group engaged in weight-bearing water-based closed kinetic chain exercises (WCKCe), and the third group participated in non-weight-bearing water-based open kinetic chain exercises (WOKCe). To uphold the integrity of the blinding process and minimize potential bias in evaluations, participants were explicitly instructed not to reveal their group assignments to the assessors [57, 65, 66].
Before the study began, all participants received a thorough briefing outlining the research objectives and methodologies, which included a section to ensure complete understanding. Consent forms were voluntarily signed by participants and/or their legal guardians in accordance with the Helsinki Declaration [67-69]. Prior to signing, the forms were reviewed to guarantee clarity and comprehension. This trial received approval from the Ethics Committee for Human Research at Bu-Ali Sina University and was registered under Iranian Registry of Clinical Trials (IRCT).
Participants
To achieve an effect size of 0.25, with a significance level of 0.05 and a statistical power of 0.8 for accurate sample size calculations, the study utilized G*Power software [70]. Previous research that employed analysis of covariance (ANCOVA), analyzing both within-group and between-group variables, guided the selection of these parameters [70-72]. The study took into account the interactions of various factors and their impacts on the outcomes. The statistical analysis, which included a power calculation of 80% and an alpha level of 0.05, indicated that a minimum of 42 patients was required to obtain reliable results [25, 73]. In consultation with a medical expert, the researcher concluded that an optimal sample size of 60 participants would be ideal to minimize potential dropout [25].
The subjects in this randomized controlled trial comprised 60 men aged between 40 and 60 years (mean age: 48.1±5.97 years). The experimental groups participated in WOKCe and WCKCe three times a week for eight weeks, in contrast to the control group, which received no intervention (Figure 1).
 Eligibility criteria required participants to be aged 40 to 60 years, have experienced CLBP for over 12 weeks, and have no prior surgeries on the hip or spine. Exclusion criteria included discomfort in various regions, irregularities in the lower and upper limbs, spondylolysis, neuromuscular disorders, and respiratory conditions [44, 74].
Eligibility criteria required participants to be aged 40 to 60 years, have experienced CLBP for over 12 weeks, and have no prior surgeries on the hip or spine. Exclusion criteria included discomfort in various regions, irregularities in the lower and upper limbs, spondylolysis, neuromuscular disorders, and respiratory conditions [44, 74].
Intervention: Water kinetic chain exercises
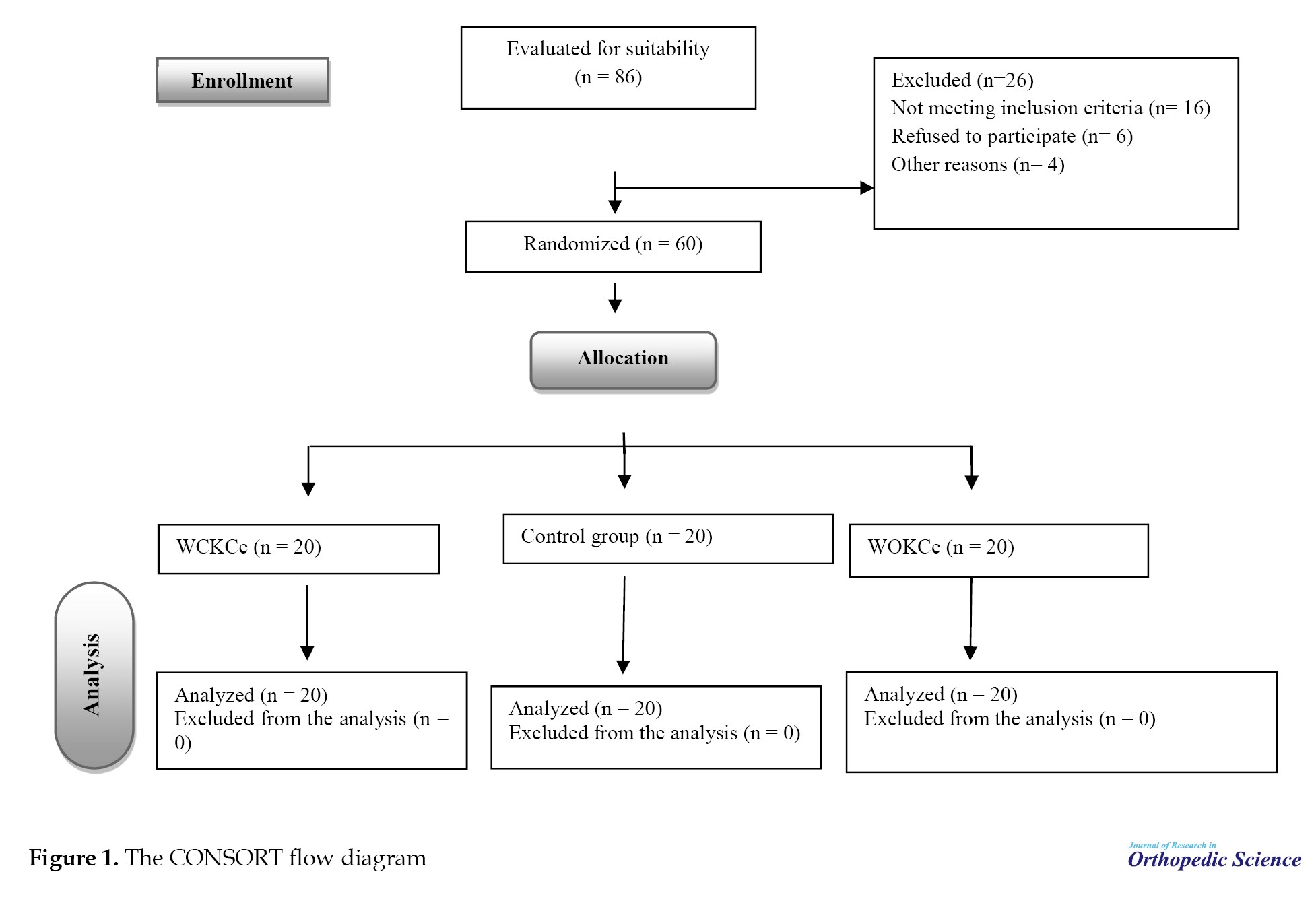
Over an eight-week period, the techniques of non-weight-bearing WOKCe and weight-bearing WCKCe were implemented in water, with participants attending three sessions per week, each lasting 60 minutes. The sessions were conducted under the supervision of the researcher and an aquatic therapy specialist. Each session commenced with a 5-minute warm-up, followed by 50 minutes dedicated to kinetic chain exercises, and concluded with a 5-minute cool-down stretching routine. Participants in the HOKCe group engaged in deep-water exercises utilizing flotation noodles, while the WCKCe group performed exercises in the shallow end of the pool, where the water level reached their xiphoid process. Aquatic therapy sessions for both groups were held at the pool of Bu-Ali Sina University in Hamadan, led by a qualified expert. The development of a phased training program for these groups was informed by previous research on volume, intensity, duration, and repetitions, with a systematic increase in exercise load implemented each week. The arrangement of WOKCe and WCKCe in the aquatic environment followed a phased approach, shaped by prior studies and the investigator’s design (Tables 1) [44, 75, 76].
MVIC
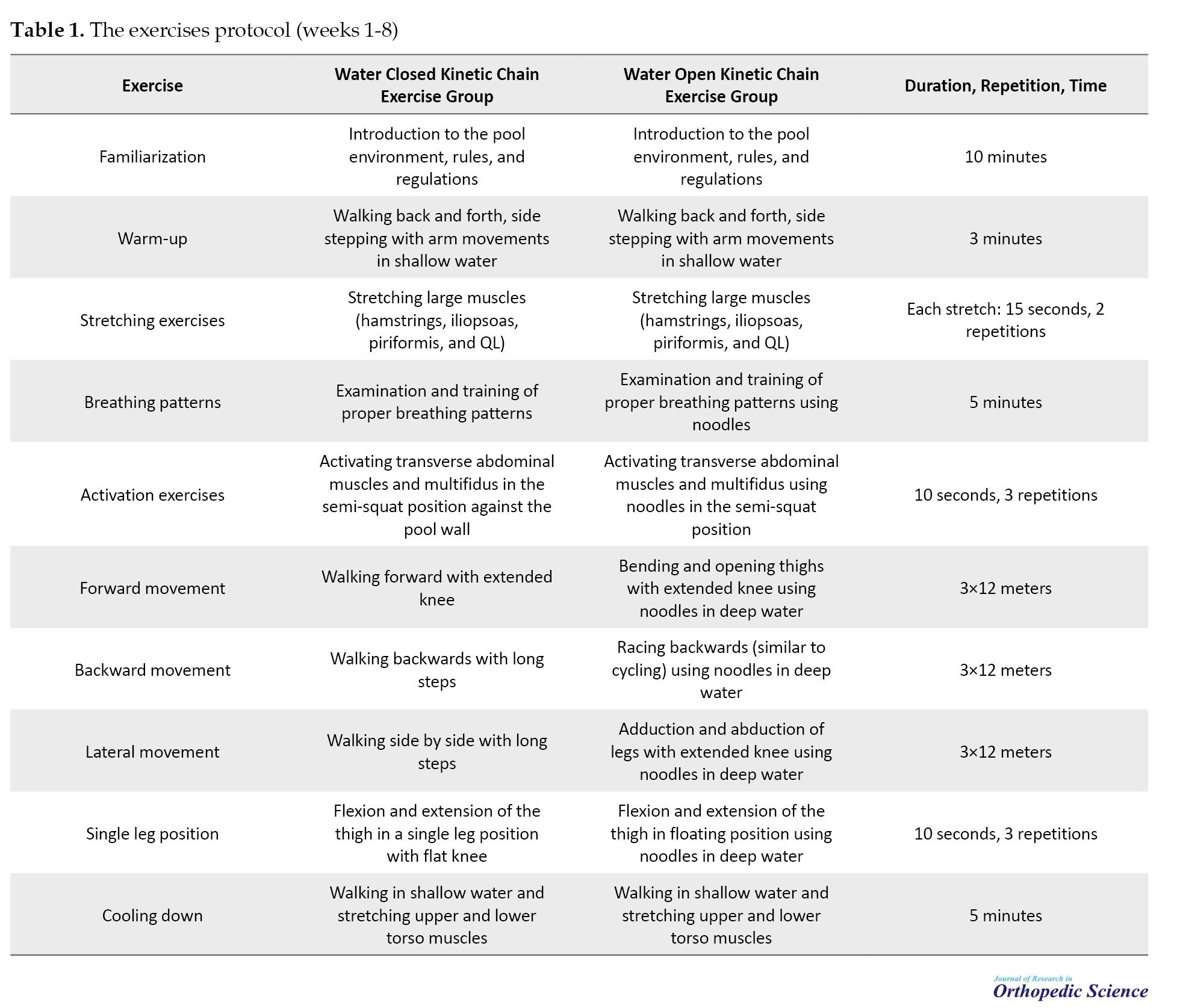
Muscle electromyographic activity measurements were obtained using Megawin’s (Finland) model ME6000, an 8-channel electromyography device (1000 Hz sampling rate) [77]. Muscle electrical activity was recorded using silver chloride passive electrodes [78]. Following skin preparation with medical alcohol, electrodes were positioned according to the SENIAM protocol on the GMed muscle, placed at the midpoint between the greater trochanter of the femur and the outermost aspect of the iliac crest after hair removal (Figure 2) [57, 79].
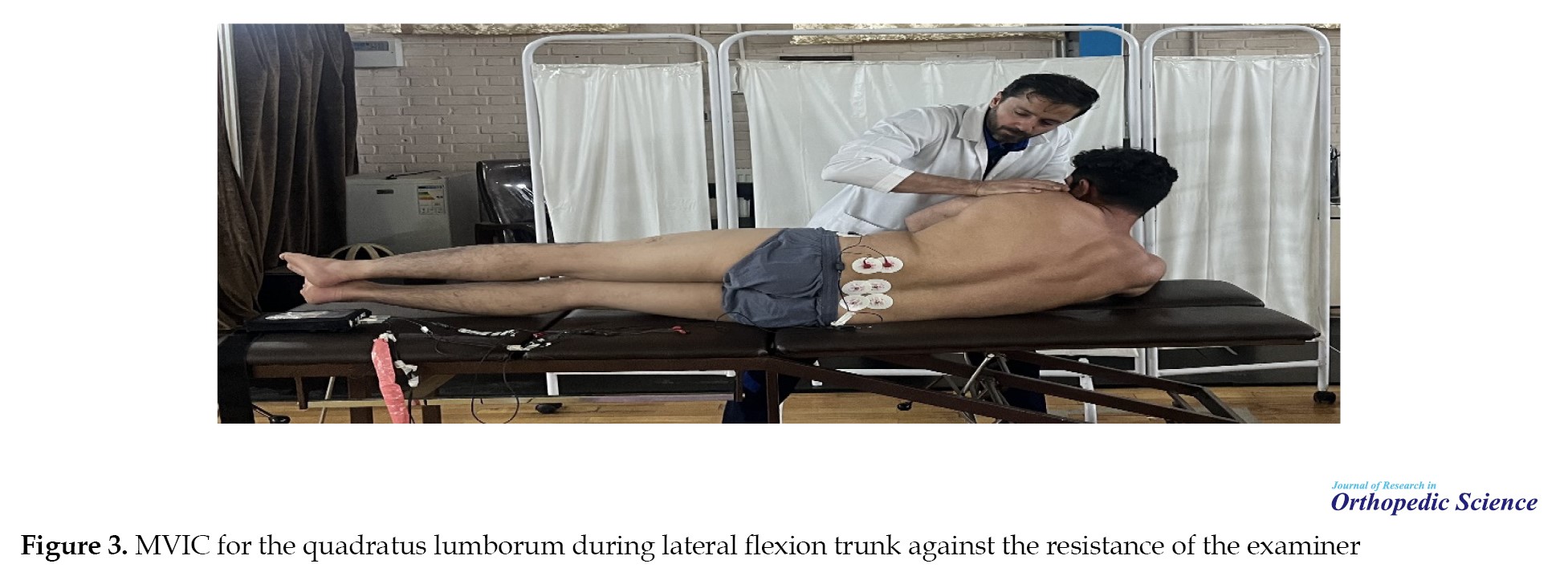
 MVIC of the QL muscle was positioned at the midpoint between the twelfth rib and the iliac crest [57, 80]. The MVIC for the GMed muscle involved an abduction movement of the thigh against the resistance of the examiner. Following the placement of electrodes at the site of the GMed muscle, the participant lay in a prone position on the examination table. Upon command, the participant performed the abduction movement of the leg toward the side (abduction) without bending the knee, as illustrated in Figure 2. The duration of this test was 5 seconds, during which three maximum isometric contractions were executed, with one-minute rest intervals between each contraction for the dominant side [57, 80-82]. The MVIC for the QL muscle involved a lateral flexion movement against the resistance of the examiner. Following the placement of electrodes at the site of the muscle, the participant lay on his side on the examination table. Upon command, the participant performed the movement against the examiner’s resistance, as illustrated in Figure 3.
MVIC of the QL muscle was positioned at the midpoint between the twelfth rib and the iliac crest [57, 80]. The MVIC for the GMed muscle involved an abduction movement of the thigh against the resistance of the examiner. Following the placement of electrodes at the site of the GMed muscle, the participant lay in a prone position on the examination table. Upon command, the participant performed the abduction movement of the leg toward the side (abduction) without bending the knee, as illustrated in Figure 2. The duration of this test was 5 seconds, during which three maximum isometric contractions were executed, with one-minute rest intervals between each contraction for the dominant side [57, 80-82]. The MVIC for the QL muscle involved a lateral flexion movement against the resistance of the examiner. Following the placement of electrodes at the site of the muscle, the participant lay on his side on the examination table. Upon command, the participant performed the movement against the examiner’s resistance, as illustrated in Figure 3.
 The duration of this test was 5 seconds, during which three maximum isometric contractions were repeated, with one-minute rest intervals between each contraction for the dominant side [57, 80-82]. Each of the MVIC movements was repeated three times, and the greatest electrical activity recorded for each muscle during the various contractions was considered the MVIC of that muscle [83, 84]. To calculate the MVIC, the muscle coactivation formula (EMGs / EMGL (EMGs + EMGL) was used [85, 86]. EMGs represent the level of activity of the muscle with lower activity, while EMGL denotes the level of activity of the muscle with higher activity during the side plank exercise [85, 86].
The duration of this test was 5 seconds, during which three maximum isometric contractions were repeated, with one-minute rest intervals between each contraction for the dominant side [57, 80-82]. Each of the MVIC movements was repeated three times, and the greatest electrical activity recorded for each muscle during the various contractions was considered the MVIC of that muscle [83, 84]. To calculate the MVIC, the muscle coactivation formula (EMGs / EMGL (EMGs + EMGL) was used [85, 86]. EMGs represent the level of activity of the muscle with lower activity, while EMGL denotes the level of activity of the muscle with higher activity during the side plank exercise [85, 86].
Statistical analyses
To evaluate the effects of the interventions on MVIC, ANCOVA was utilized, with eta-squared (η²) employed as a measure of effect size [87]. Pairwise comparisons were performed using the Bonferroni correction to control for type I error [88]. Additionally, the percentage of change (POC) from pre-test to post-test scores was calculated according to the formula established by Soufivand et al., with statistical significance set at P<0.05 [89] (Equation 1).
Results
Table 2 displays the mean demographic characteristics, including age, height, weight, and body mass index (BMI) of participants.
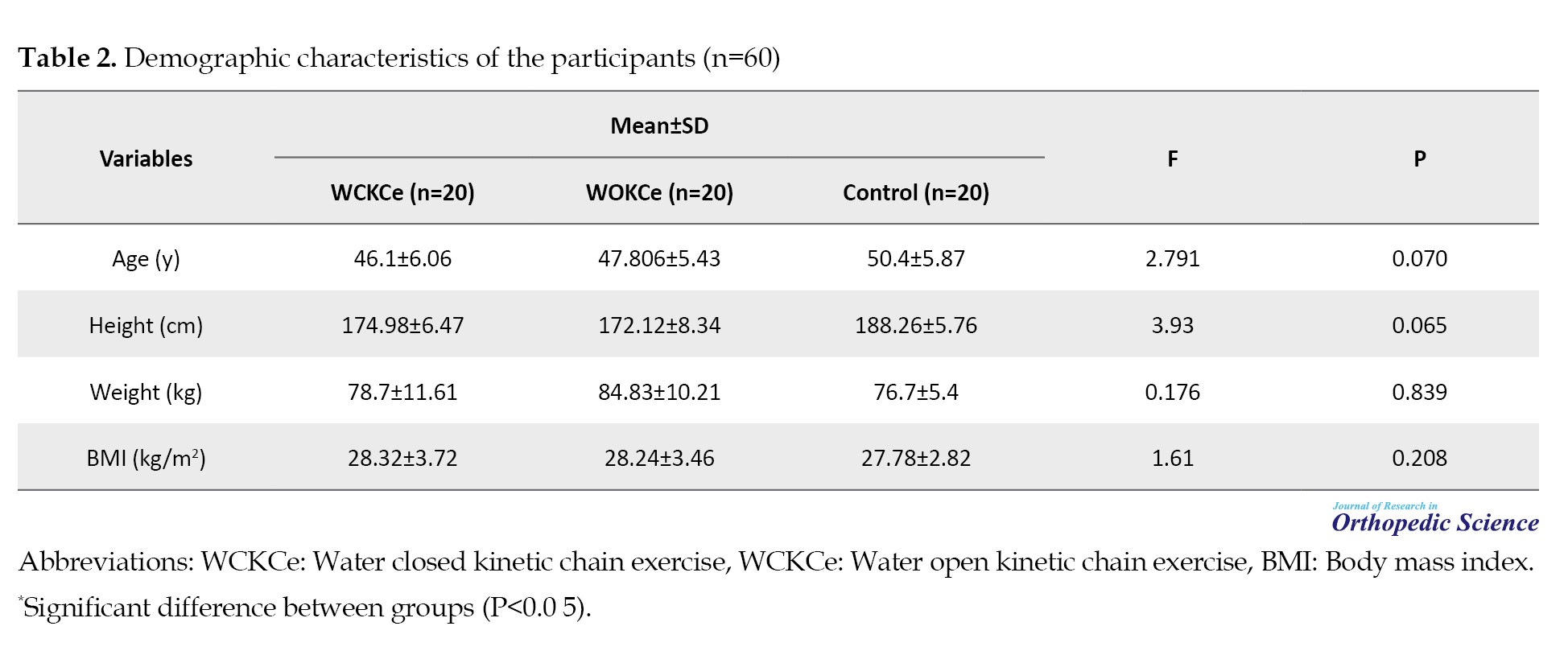
Furthermore, the results of the Shapiro-Wilk test are presented in Table 2. These results indicated that the data from the three groups—WOKCe, WCKCe, and control—were normally distributed, as demonstrated by P-values exceeding 0.05 for the research variables.
MVIC
In the WCKCe group, MVIC of the GMed muscle showed a significant improvement of 13.01% (P=0.009), indicating a positive effect of the intervention (P=0.007), suggesting effective intervention outcomes. The WOKCe group exhibited a notable improvement of 23.18% in MVIC of the QL muscle (P=0.028), indicating a strong positive effect of the treatment. Finally, the WCKCe group showed a significant improvement of 13.01% in MVIC of the QL muscle (P=0.003). In the control group, MVIC of the GMed decreased from pre-test to post-test by 5.63%; however, this change was not statistically significant (P=0.372). A similar non-significant decrease of 5.51% was observed in MVIC of the QL (P=0.186) (Table 3).
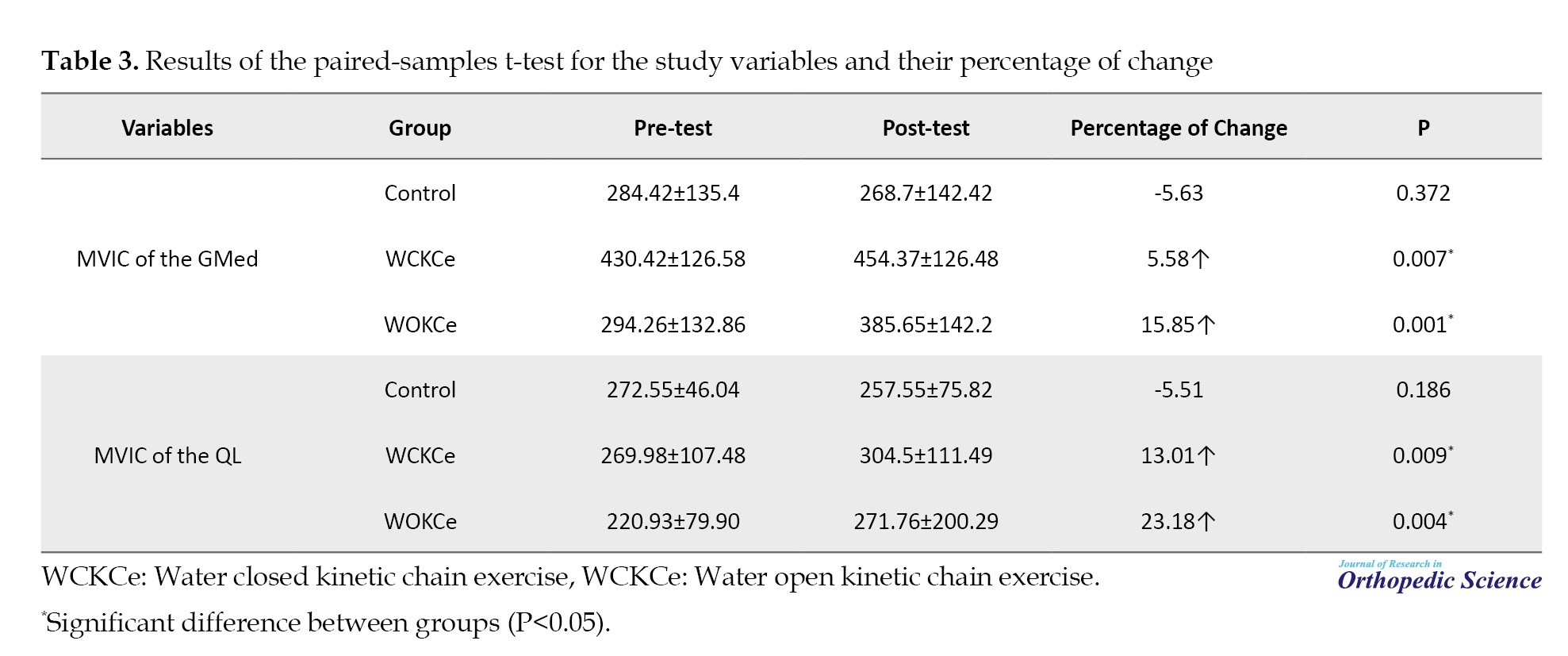
Table 4 presents the ANCOVA results, which revealed a statistically significant difference among the groups regarding the MVIC of the GMed muscle (F=7.08, P=0.002).
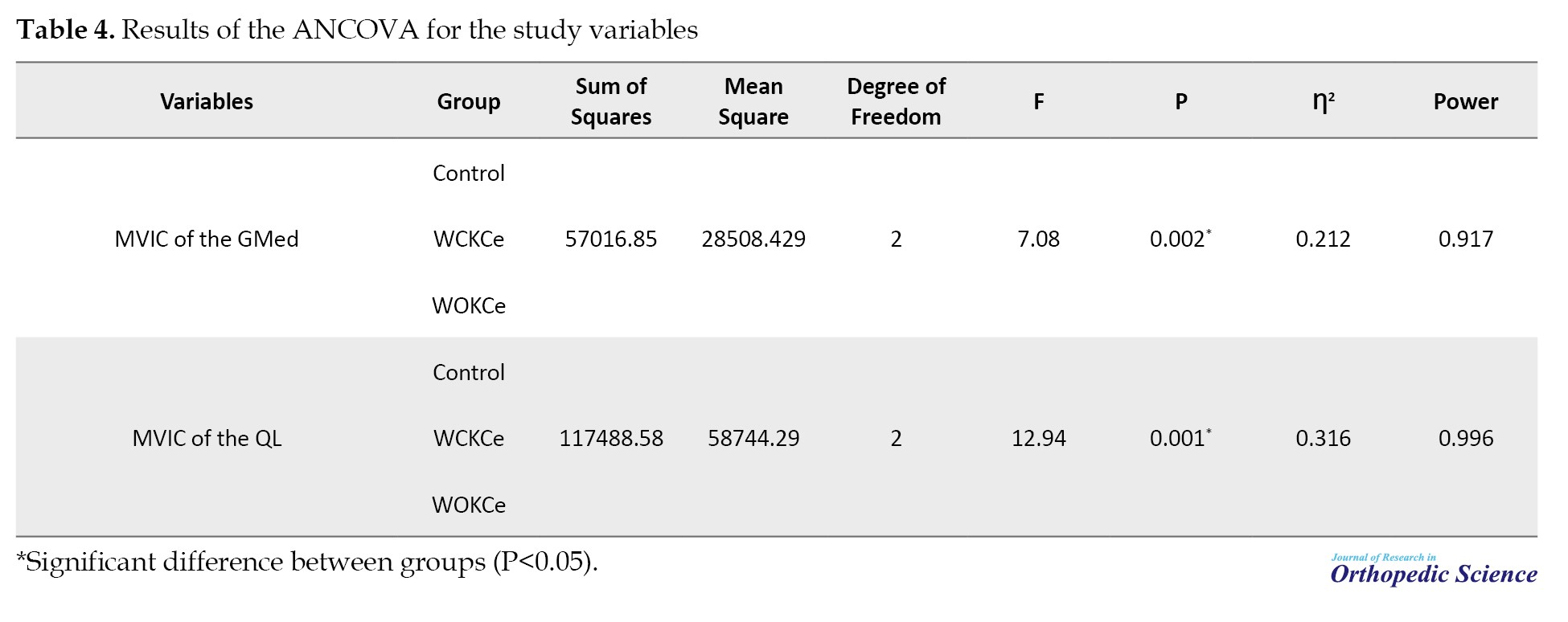
The effect size, indicated by eta-squared (Ƞ²=0.212), suggested a moderate effect, meaning that group membership accounted for a substantial portion of the variance in the MVIC of the GMed muscle. Additionally, the analysis demonstrated high statistical power (0.968), indicating a strong likelihood of detecting a true effect if one exists. Also, the ANCOVA results for the MVIC the QL muscle showed statistically significant group differences (F=12.94, P=0.001, Ƞ²=0.996). These results indicate that there is sufficient evidence to conclude significant differences in the MVIC of the GMed and QL muscles among the WCKCe, WOKCe, and control groups.
Table 5 presents a comparative analysis of the study variables across the groups, revealing several important findings.
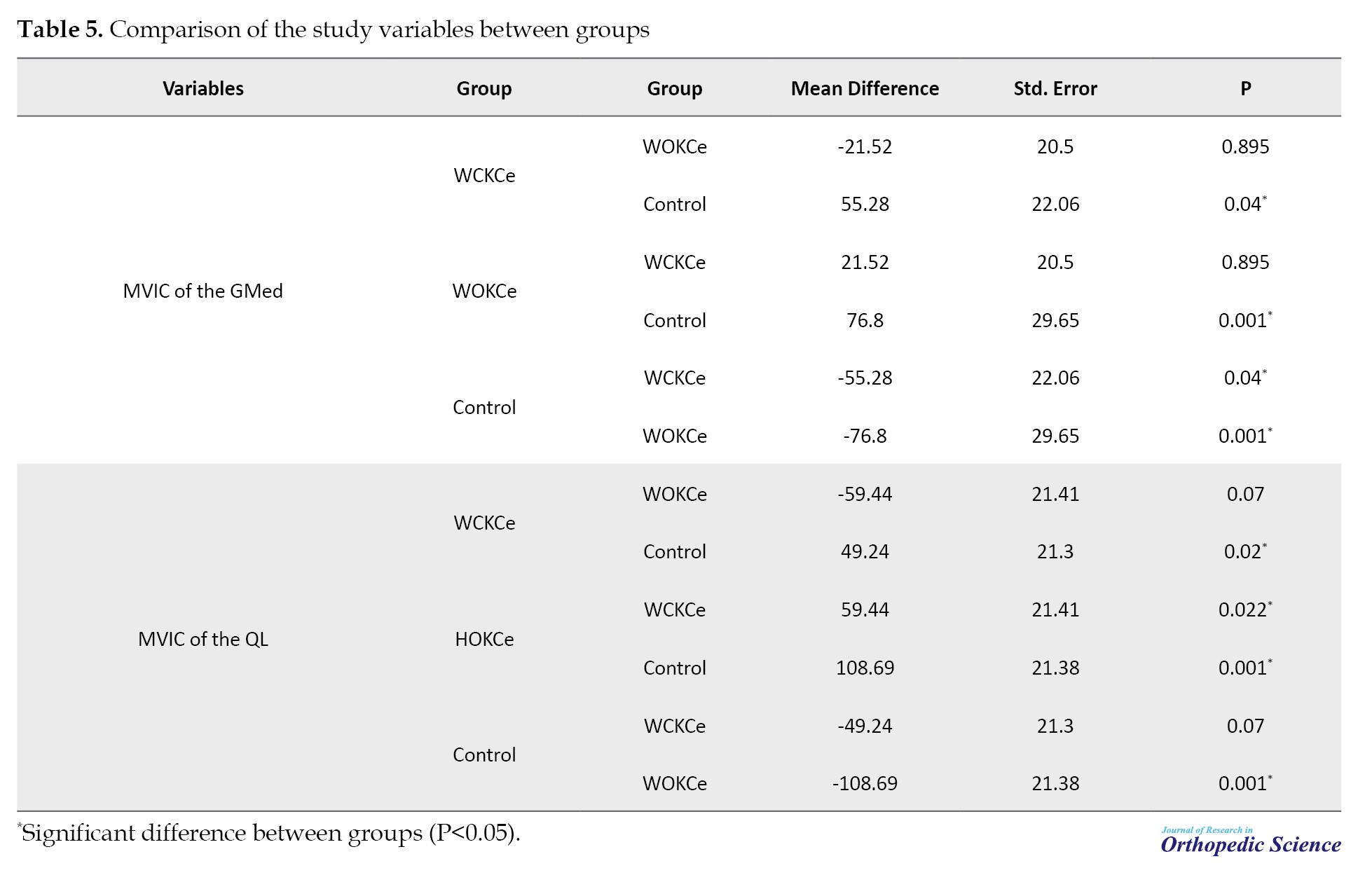
Notably, a statistically significant difference in MVIC of the GMed muscle was observed between the WCKCe group and the control group (P=0.04), as well as between the WOKCe group and the control group (P=0.001). This statistically significant result indicates a possible influence of the WCKCe and WOKCe interventions on MVIC of the GMed muscle. Furthermore, the analysis revealed that there was no statistically significant difference observed between the two experimental groups (P=0.895), suggesting that these two interventions had similar effects on this particular muscle parameter. The analysis of the MVIC of the QL muscle revealed that both the WCKCe and WOKCe groups exhibited statistically significant differences compared to the control group (P=0.02 and P=0.001, respectively). This finding suggests that the interventions had a meaningful impact on the QL muscle strength. However, there was no statistically significant difference between the WCKCe and WOKCe groups regarding the MVIC of the QL muscle (P=0.07).
Discussion
The primary objective of this study was to assess the effects of WCKCe and WOKCe on the MVIC of the gluteus GMed and QL muscles. The results demonstrated a statistically significant and positive effect of the intervention on MVIC GMed and QL muscles in the experimental groups, with improvements ranging from 5.58% to 23.18%. Consequently, the findings confirmed the efficacy of the specific training protocol in enhancing MVIC GMed and QL muscles in experimental groups. This observed enhancement in muscular strength corroborates existing literature, which attributes the efficacy of aquatic therapy to the distinct hydrodynamic properties of water, namely buoyancy and omnidirectional resistance [33, 37, 70, 76, 89- 91]. The scientific rationale for these results becomes highly specific when considering the intervention as a form of water-based resistance exercise; the unique properties of water provide a distinct physiological stimulus compared to land-based training [33, 74, 76, 92, 93]. Water provides resistance in all planes of movement, unlike gravity, which is primarily vertical [33, 61, 94-96]. This constant, multi-directional load requires sustained stabilization from the deep core muscles, particularly the quadratus QL and GMed, to maintain a neutral pelvis and spine [19, 97, 98]. Furthermore, the viscosity of water generates a velocity-dependent resistance that imposes a substantial eccentric load during movement deceleration, a potent stimulus for neuromuscular adaptation and strength gain [76, 99, 100]. This environment of turbulence and omnidirectional perturbation constantly challenges postural control, thereby heightening proprioceptive input to the central nervous system [40, 61, 76, 95, 101]. In response to this heightened demand, the body augments motor unit recruitment to key lumbo-pelvic stabilizers, such as the GMed for hip and pelvic control, and the QL for lumbar stabilization directly resulting in the observed significant improvements in maximum voluntary contraction [90, 97, 102-105]. The buoyancy of water significantly reduces compressive forces on the spine and joints that this character allows for a higher training volume and greater range of motion with less pain or fatigue [32, 40, 59, 70, 91, 96, 97]. In summary, the combination of multi-directional resistance, enhanced proprioceptive challenge, and a low-impact environment created an ideal stimulus for neuromuscular adaptation in the lumbo-pelvic stabilizers, resulting in the significant strength gains observed in the intervention groups [61, 76, 97, 100, 106].
The implementation of WCKCe has been shown to significantly enhance proprioceptive input and neuromuscular control, which likely contributed to the observed strength gains in muscles of GMed and QL. Research by Bunton et al., Irish et al., Sciascia and Cromwell, and Tang et al. supports this assertion, indicating that closed-chain movements engage multiple muscle groups and joint stabilizers, thereby fostering a more integrated neuromuscular response [48, 53, 56, 107]. This type of exercise promotes dynamic stability and coordination, which are critical for effective movement patterns and injury prevention [48, 53, 56, 107]. In contrast, WOKCe have their own unique benefits, particularly in terms of facilitating a greater range of motion and promoting isolated muscle activation. Studies conducted by Lephart and Henry, Lust, Öberg et al., and Sciascia and Cromwell highlight that open chain exercises allow for targeted strengthening of specific muscles without the influence of surrounding muscle groups [50, 52, 53, 108]. This isolation can be particularly beneficial for rehabilitation purposes, where focused muscle activation is necessary to restore function and strength [28]. Enhancing the MVIC of the GMed and QL muscles is essential for improving overall lower limb function and preventing injuries [22, 24, 29]. One effective method for achieving this is through resistance exercises utilizing a theraband resistance bands (TRB) in water [57]. Resistance training, particularly when incorporating tools such as the TRB, provides a unique approach to muscle activation [109, 110]. The TRB offers variable resistance that can be adjusted according to the individual’s strength level and rehabilitation needs [102]. This synergy is particularly advantageous for targeting the GMed and QL muscles due to a dual-mechanism approach. First, buoyancy mitigates joint compressive and gravitational forces, permitting greater range of motion and training volume with reduced pain and inhibitory feedback [58, 102, 111]. Second, the TRB provides targeted, elastic resistance in specific planes of movement (e.g. hip abduction), which directly and intensively engages the GMed without placing the joints under high axial loads [104, 112]. This combination creates an ideal high-stimulus, low-stress environment for neuromuscular adaptation [33, 60, 90, 97].
Studies have shown that performing resistance exercises in water can lead to increased MVIC levels due to the unique resistance properties of water [32, 70], which challenge the muscle fibers differently compared to land-based exercises [95, 96]. The inherent instability of the aquatic environment provides a continuous challenge to postural control, which heightens proprioceptive feedback to the central nervous system [103, 105]. This enhanced sensory input is essential for refining the neuromuscular control and coordination of movements involving the GMed, thereby increasing the overall effectiveness of the training regimen [58, 113]. To optimize increases in the MVIC of the GMed using TRB resistance in an aquatic environment, specific exercise prescriptions are fundamental [33, 60, 103]. A primary example involves performing standing lateral leg raises with a TRB secured around the ankles [102, 103, 109, 114]. This configuration effectively targets the GMed by superimposing the elastic resistance of the band onto the hydrodynamic resistance of water, thereby creating a compounded stimulus for muscle engagement [57, 102, 103, 109, 114]. This synergistic loading mechanism directly facilitates significant improvements in both GMed strength and lumbo-pelvic stability [104, 105, 110, 111]. Enhanced strength in the GMed and QL is foundational for improved balance, stability, and overall physical performance, which are critical for individuals in rehabilitation [29].
The ANCOVA results indicate no significant differential effect of exercise type on MVIC of the GMed between the WCKCe and WOKCe groups (P=0.895), demonstrating that both modalities were equally effective in improving GMed MVIC. This finding supports the concept that the distinction between closed and open kinetic chain exercises may not substantially influence strength outcomes in this population. Regarding MVIC of the QL muscle, both interventions again produced significant improvements relative to the control group, with the WCKCe group achieving a 13.01% increase (P=0.009) and the WOKCe group a 23.18% gain (P=0.004), confirming the efficacy of both modalities for targeting this crucial core stabilizer. Consistent with the GMed findings, no statistically significant difference emerged between the two intervention groups for MVIC of the QL (P=0.07). This consistent pattern across both muscles reinforces that WCKCe and WOKCe provide comparable benefits for enhancing lumbo-pelvic stabilizer strength, offering clinicians flexibility in exercise selection.
The underlying mechanisms for strength improvement in both muscles may involve similar neuromuscular adaptations, as both exercise types engage overlapping muscle groups and movement patterns [26, 29, 79, 103]. The comparative analysis of WCKCe and WOKCe reveals important implications for rehabilitation practices. Both exercise modalities leverage the unique properties of water to enhance muscle strength while minimizing the risk of injury associated with traditional land-based exercises [32, 33, 70]. Moreover, the findings suggest that clinicians can confidently implement either WCKCe or WOKCe in rehabilitation programs, depending on individual patient needs and preferences. For instance, WCKCe may be more suitable for patients requiring stability and support [44, 49, 50, 56, 108], while WOKCe could be advantageous for those aiming to enhance functional mobility and strength through a broader range of motion [53, 58]. The implications of these findings extend beyond immediate muscle strength improvements. Enhanced strength in the GMed and QL muscles is associated with improved functional outcomes, including better balance, stability, and overall physical performance. These factors are critical for athletes returning to sport and for individuals seeking to maintain an active lifestyle post-rehabilitation. The combination of TRB with hydrodynamic loading is particularly effective. Clinicians may freely choose between WCKCe and WOKCe for improving GMed and QL strength, as both yield comparable results. This provides flexibility to tailor programs to individual patient preferences and functional goals. This approach is especially beneficial for patients requiring low-impact training, such as those with LBP, hip pathologies, or during post-operative rehabilitation. Aquatic exercise offers an effective, flexible, and joint-protective approach to enhancing lumbo-pelvic stability and function.
This study has several limitations that should be addressed in future research. First, the long-term efficacy of both WCKCe and WOKCe on maintained strength improvements and functional outcomes remains unexplored. Second, the underlying neuromuscular adaptations, such as changes in motor unit recruitment patterns and muscle activation timing were not investigated. Additionally, the impact of these interventions on quality-of-life measures across diverse clinical populations warrants examination. Future studies should also establish optimal rehabilitation parameters by examining dose-response relationships through varied exercise intensities, durations, and frequencies. These investigations would substantiate the implementation of aquatic exercises as a primary strengthening modality rather than solely an initial rehabilitation approach.
Conclusion
Our study highlights the effectiveness of an 8-week aquatic exercise program in strengthening core muscles among men with CNSLBP. For clinicians, this underscores the importance of integrating aquatic therapy into rehabilitation strategies to enhance patient outcomes, including pain reduction and improved functional mobility. It is crucial for healthcare providers to tailor these interventions to individual patient needs and consider the study’s limitations when applying the findings. Future investigations should focus on the long-term effects and broader applicability of aquatic exercises in diverse patient populations to optimize low back pain management. Clinicians can select WCKCe or WOKCe considering patient mobility and preference without compromising strength gains.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee for Human Research at Bu-Ali Sina University, Hamadan, Iran (Code: IR.BASU.REC.1402.011). This study was registered by the Iranian Registry of Clinical Trials (IRCT) (Code: IRCT.20190129042534N1). Before experimental procedures began, all the participants reviewed and voluntarily signed an informed written consent form.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study design, and writing: Ali Yalfani; Data interpretation: Hossien Ashoury; Data acquisition, and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all participants in this study.
References
Chronic low back pain (CLBP) is a widespread condition that significantly impacts the lives of millions of individuals worldwide, often leading to physical limitations and diminished quality of life (QoL) [1-5]. It is characterized by persistent discomfort in the lower back that lasts for more than three months and can arise from various factors, including muscular imbalances, poor posture, and previous injuries [6-8]. The maximum voluntary isometric contraction (MVIC) is the peak force or torque a muscle group can generate in a single maximal effort against an immovable resistance [9-11]. It is a key measure in strength and conditioning, used to assess muscle function and track progress in training or rehabilitation [9, 12]. Studies suggest that weakened stabilizing muscles’ MVIC may contribute to instability and discomfort in individuals with CLBP [13-15]. Evaluating MVIC in the lumbar region helps identify deficits that may exacerbate CLBP and guide targeted rehabilitation strategies [12-15]. For instance, when larger and stronger muscles are activated first without proper assistance from smaller stabilizing muscles, this disparity may overload the lumbar structures and ultimately cause discomfort or pain [16]. Additionally, the regular application of an unsuitable activation sequence can lead to muscle fatigue, weakness, and a heightened injury risk, underscoring the necessity for correct movement mechanics and muscle coordination in averting CLBP [17]. Among the key contributors to CLBP are dysfunctions in the stabilizing muscles of the lumbar and pelvic regions, particularly the gluteus medius (GMed) and quadratus lumborum (QL) [18-20]. Impairments in the strength and coordination of these muscles can lead to altered biomechanics [21, 22], resulting in increased stress on the lumbar spine and contributing to the persistence of CLBP [23-28]. Their synergistic activation is essential for maintaining optimal pelvic alignment and spinal integrity during dynamic activities, thereby preventing compensatory movement patterns and reducing the risk of musculoskeletal injuries [22, 29]. Function coordination of these muscles is essential for maintaining pelvic stability and proper spinal alignment during movement [10, 24-26]. In general, adequate strengthening and coordination of the QL and GMed muscles can enhance muscular health and establish a stable base for the lower back, assisting in the prevention of CLBP [30].
Conventional rehabilitation methods typically emphasize the importance of strengthening essential muscles [19, 31]. However, numerous patients find it challenging to consistently engage in land-based exercise programs, often due to discomfort or concerns about worsening their condition [32-34]. Water-based exercise programs have emerged as a promising solution, leveraging the unique properties of water to create a supportive environment that reduces joint stress while providing resistance for muscle strengthening [6, 32, 35-42]. he human body should not be viewed as a collection of isolated muscles, bones, connective tissues, and ligaments; rather, it is an integrated system where each component influences the others, and this interaction can yield either beneficial or detrimental effects [43-50]. Ideally, when the motor chain is engaged, the body operates as a cohesive unit, facilitating smooth and efficient movements [50-54].
Water kinetic chain exercises (WKCe) utilize the buoyancy and resistance of water to facilitate movement patterns that mimic functional activities, allowing individuals to engage in exercises with reduced pain and increased range of motion [45, 47, 55- 58]. Despite the potential advantages of aquatic therapy, there remains a significant gap in the literature regarding its specific effects on muscle activation in patients with CLBP [59-62].
The lack of research underscores the necessity for systematic investigation into the efficacy of WKCe on performance. The present study aimed to explore the impact of WKCe on MVIC of the GMed and QL muscles in individuals suffering from chronic non-specific low back pain (CNSLBP). By comparing the outcomes of both intervention groups, this research sought to determine whether WKCe can provide superior benefits in enhancing muscle function and alleviating pain levels. The findings from this investigation could significantly inform clinical practice, encouraging the integration of aquatic exercise into treatment plans for CNSLBP. Ultimately, this research aspires to contribute to the growing body of evidence supporting innovative rehabilitation strategies, offering hope for improved recovery and enhanced QoL for individuals affected by CNSLBP. By addressing this significant health issue, the study aimed to pave the way for more effective, patient-centered rehabilitation approaches that meet the needs of those suffering from this debilitating condition.
Methods
The present study employed a double-blind, randomized controlled pilot design to examine the effects of an intervention on individuals suffering from CNSLBP. To ensure reliable outcome assessments, comprehensive data collection was conducted both before and after the trial, incorporating subjective feedback and physiological evaluations [57]. Randomization was achieved by generating codes in blocks of four and six using Random Allocation Software, version 1.0 [63]. The allocation process was concealed with sequentially numbered, opaque, sealed envelopes, which were intentionally substantial to highlight their importance [64]. An orthopedic specialist diagnosed participants with CNSLBP following MRI scans and physical examinations. Sixty participants were randomly assigned to three groups of twenty to maintain balance within the study. One group served as the control, while another group engaged in weight-bearing water-based closed kinetic chain exercises (WCKCe), and the third group participated in non-weight-bearing water-based open kinetic chain exercises (WOKCe). To uphold the integrity of the blinding process and minimize potential bias in evaluations, participants were explicitly instructed not to reveal their group assignments to the assessors [57, 65, 66].
Before the study began, all participants received a thorough briefing outlining the research objectives and methodologies, which included a section to ensure complete understanding. Consent forms were voluntarily signed by participants and/or their legal guardians in accordance with the Helsinki Declaration [67-69]. Prior to signing, the forms were reviewed to guarantee clarity and comprehension. This trial received approval from the Ethics Committee for Human Research at Bu-Ali Sina University and was registered under Iranian Registry of Clinical Trials (IRCT).
Participants
To achieve an effect size of 0.25, with a significance level of 0.05 and a statistical power of 0.8 for accurate sample size calculations, the study utilized G*Power software [70]. Previous research that employed analysis of covariance (ANCOVA), analyzing both within-group and between-group variables, guided the selection of these parameters [70-72]. The study took into account the interactions of various factors and their impacts on the outcomes. The statistical analysis, which included a power calculation of 80% and an alpha level of 0.05, indicated that a minimum of 42 patients was required to obtain reliable results [25, 73]. In consultation with a medical expert, the researcher concluded that an optimal sample size of 60 participants would be ideal to minimize potential dropout [25].
The subjects in this randomized controlled trial comprised 60 men aged between 40 and 60 years (mean age: 48.1±5.97 years). The experimental groups participated in WOKCe and WCKCe three times a week for eight weeks, in contrast to the control group, which received no intervention (Figure 1).
Intervention: Water kinetic chain exercises
Over an eight-week period, the techniques of non-weight-bearing WOKCe and weight-bearing WCKCe were implemented in water, with participants attending three sessions per week, each lasting 60 minutes. The sessions were conducted under the supervision of the researcher and an aquatic therapy specialist. Each session commenced with a 5-minute warm-up, followed by 50 minutes dedicated to kinetic chain exercises, and concluded with a 5-minute cool-down stretching routine. Participants in the HOKCe group engaged in deep-water exercises utilizing flotation noodles, while the WCKCe group performed exercises in the shallow end of the pool, where the water level reached their xiphoid process. Aquatic therapy sessions for both groups were held at the pool of Bu-Ali Sina University in Hamadan, led by a qualified expert. The development of a phased training program for these groups was informed by previous research on volume, intensity, duration, and repetitions, with a systematic increase in exercise load implemented each week. The arrangement of WOKCe and WCKCe in the aquatic environment followed a phased approach, shaped by prior studies and the investigator’s design (Tables 1) [44, 75, 76].
MVIC
Muscle electromyographic activity measurements were obtained using Megawin’s (Finland) model ME6000, an 8-channel electromyography device (1000 Hz sampling rate) [77]. Muscle electrical activity was recorded using silver chloride passive electrodes [78]. Following skin preparation with medical alcohol, electrodes were positioned according to the SENIAM protocol on the GMed muscle, placed at the midpoint between the greater trochanter of the femur and the outermost aspect of the iliac crest after hair removal (Figure 2) [57, 79].
Statistical analyses
To evaluate the effects of the interventions on MVIC, ANCOVA was utilized, with eta-squared (η²) employed as a measure of effect size [87]. Pairwise comparisons were performed using the Bonferroni correction to control for type I error [88]. Additionally, the percentage of change (POC) from pre-test to post-test scores was calculated according to the formula established by Soufivand et al., with statistical significance set at P<0.05 [89] (Equation 1).
Results
Table 2 displays the mean demographic characteristics, including age, height, weight, and body mass index (BMI) of participants.
Furthermore, the results of the Shapiro-Wilk test are presented in Table 2. These results indicated that the data from the three groups—WOKCe, WCKCe, and control—were normally distributed, as demonstrated by P-values exceeding 0.05 for the research variables.
MVIC
In the WCKCe group, MVIC of the GMed muscle showed a significant improvement of 13.01% (P=0.009), indicating a positive effect of the intervention (P=0.007), suggesting effective intervention outcomes. The WOKCe group exhibited a notable improvement of 23.18% in MVIC of the QL muscle (P=0.028), indicating a strong positive effect of the treatment. Finally, the WCKCe group showed a significant improvement of 13.01% in MVIC of the QL muscle (P=0.003). In the control group, MVIC of the GMed decreased from pre-test to post-test by 5.63%; however, this change was not statistically significant (P=0.372). A similar non-significant decrease of 5.51% was observed in MVIC of the QL (P=0.186) (Table 3).
Table 4 presents the ANCOVA results, which revealed a statistically significant difference among the groups regarding the MVIC of the GMed muscle (F=7.08, P=0.002).
The effect size, indicated by eta-squared (Ƞ²=0.212), suggested a moderate effect, meaning that group membership accounted for a substantial portion of the variance in the MVIC of the GMed muscle. Additionally, the analysis demonstrated high statistical power (0.968), indicating a strong likelihood of detecting a true effect if one exists. Also, the ANCOVA results for the MVIC the QL muscle showed statistically significant group differences (F=12.94, P=0.001, Ƞ²=0.996). These results indicate that there is sufficient evidence to conclude significant differences in the MVIC of the GMed and QL muscles among the WCKCe, WOKCe, and control groups.
Table 5 presents a comparative analysis of the study variables across the groups, revealing several important findings.
Notably, a statistically significant difference in MVIC of the GMed muscle was observed between the WCKCe group and the control group (P=0.04), as well as between the WOKCe group and the control group (P=0.001). This statistically significant result indicates a possible influence of the WCKCe and WOKCe interventions on MVIC of the GMed muscle. Furthermore, the analysis revealed that there was no statistically significant difference observed between the two experimental groups (P=0.895), suggesting that these two interventions had similar effects on this particular muscle parameter. The analysis of the MVIC of the QL muscle revealed that both the WCKCe and WOKCe groups exhibited statistically significant differences compared to the control group (P=0.02 and P=0.001, respectively). This finding suggests that the interventions had a meaningful impact on the QL muscle strength. However, there was no statistically significant difference between the WCKCe and WOKCe groups regarding the MVIC of the QL muscle (P=0.07).
Discussion
The primary objective of this study was to assess the effects of WCKCe and WOKCe on the MVIC of the gluteus GMed and QL muscles. The results demonstrated a statistically significant and positive effect of the intervention on MVIC GMed and QL muscles in the experimental groups, with improvements ranging from 5.58% to 23.18%. Consequently, the findings confirmed the efficacy of the specific training protocol in enhancing MVIC GMed and QL muscles in experimental groups. This observed enhancement in muscular strength corroborates existing literature, which attributes the efficacy of aquatic therapy to the distinct hydrodynamic properties of water, namely buoyancy and omnidirectional resistance [33, 37, 70, 76, 89- 91]. The scientific rationale for these results becomes highly specific when considering the intervention as a form of water-based resistance exercise; the unique properties of water provide a distinct physiological stimulus compared to land-based training [33, 74, 76, 92, 93]. Water provides resistance in all planes of movement, unlike gravity, which is primarily vertical [33, 61, 94-96]. This constant, multi-directional load requires sustained stabilization from the deep core muscles, particularly the quadratus QL and GMed, to maintain a neutral pelvis and spine [19, 97, 98]. Furthermore, the viscosity of water generates a velocity-dependent resistance that imposes a substantial eccentric load during movement deceleration, a potent stimulus for neuromuscular adaptation and strength gain [76, 99, 100]. This environment of turbulence and omnidirectional perturbation constantly challenges postural control, thereby heightening proprioceptive input to the central nervous system [40, 61, 76, 95, 101]. In response to this heightened demand, the body augments motor unit recruitment to key lumbo-pelvic stabilizers, such as the GMed for hip and pelvic control, and the QL for lumbar stabilization directly resulting in the observed significant improvements in maximum voluntary contraction [90, 97, 102-105]. The buoyancy of water significantly reduces compressive forces on the spine and joints that this character allows for a higher training volume and greater range of motion with less pain or fatigue [32, 40, 59, 70, 91, 96, 97]. In summary, the combination of multi-directional resistance, enhanced proprioceptive challenge, and a low-impact environment created an ideal stimulus for neuromuscular adaptation in the lumbo-pelvic stabilizers, resulting in the significant strength gains observed in the intervention groups [61, 76, 97, 100, 106].
The implementation of WCKCe has been shown to significantly enhance proprioceptive input and neuromuscular control, which likely contributed to the observed strength gains in muscles of GMed and QL. Research by Bunton et al., Irish et al., Sciascia and Cromwell, and Tang et al. supports this assertion, indicating that closed-chain movements engage multiple muscle groups and joint stabilizers, thereby fostering a more integrated neuromuscular response [48, 53, 56, 107]. This type of exercise promotes dynamic stability and coordination, which are critical for effective movement patterns and injury prevention [48, 53, 56, 107]. In contrast, WOKCe have their own unique benefits, particularly in terms of facilitating a greater range of motion and promoting isolated muscle activation. Studies conducted by Lephart and Henry, Lust, Öberg et al., and Sciascia and Cromwell highlight that open chain exercises allow for targeted strengthening of specific muscles without the influence of surrounding muscle groups [50, 52, 53, 108]. This isolation can be particularly beneficial for rehabilitation purposes, where focused muscle activation is necessary to restore function and strength [28]. Enhancing the MVIC of the GMed and QL muscles is essential for improving overall lower limb function and preventing injuries [22, 24, 29]. One effective method for achieving this is through resistance exercises utilizing a theraband resistance bands (TRB) in water [57]. Resistance training, particularly when incorporating tools such as the TRB, provides a unique approach to muscle activation [109, 110]. The TRB offers variable resistance that can be adjusted according to the individual’s strength level and rehabilitation needs [102]. This synergy is particularly advantageous for targeting the GMed and QL muscles due to a dual-mechanism approach. First, buoyancy mitigates joint compressive and gravitational forces, permitting greater range of motion and training volume with reduced pain and inhibitory feedback [58, 102, 111]. Second, the TRB provides targeted, elastic resistance in specific planes of movement (e.g. hip abduction), which directly and intensively engages the GMed without placing the joints under high axial loads [104, 112]. This combination creates an ideal high-stimulus, low-stress environment for neuromuscular adaptation [33, 60, 90, 97].
Studies have shown that performing resistance exercises in water can lead to increased MVIC levels due to the unique resistance properties of water [32, 70], which challenge the muscle fibers differently compared to land-based exercises [95, 96]. The inherent instability of the aquatic environment provides a continuous challenge to postural control, which heightens proprioceptive feedback to the central nervous system [103, 105]. This enhanced sensory input is essential for refining the neuromuscular control and coordination of movements involving the GMed, thereby increasing the overall effectiveness of the training regimen [58, 113]. To optimize increases in the MVIC of the GMed using TRB resistance in an aquatic environment, specific exercise prescriptions are fundamental [33, 60, 103]. A primary example involves performing standing lateral leg raises with a TRB secured around the ankles [102, 103, 109, 114]. This configuration effectively targets the GMed by superimposing the elastic resistance of the band onto the hydrodynamic resistance of water, thereby creating a compounded stimulus for muscle engagement [57, 102, 103, 109, 114]. This synergistic loading mechanism directly facilitates significant improvements in both GMed strength and lumbo-pelvic stability [104, 105, 110, 111]. Enhanced strength in the GMed and QL is foundational for improved balance, stability, and overall physical performance, which are critical for individuals in rehabilitation [29].
The ANCOVA results indicate no significant differential effect of exercise type on MVIC of the GMed between the WCKCe and WOKCe groups (P=0.895), demonstrating that both modalities were equally effective in improving GMed MVIC. This finding supports the concept that the distinction between closed and open kinetic chain exercises may not substantially influence strength outcomes in this population. Regarding MVIC of the QL muscle, both interventions again produced significant improvements relative to the control group, with the WCKCe group achieving a 13.01% increase (P=0.009) and the WOKCe group a 23.18% gain (P=0.004), confirming the efficacy of both modalities for targeting this crucial core stabilizer. Consistent with the GMed findings, no statistically significant difference emerged between the two intervention groups for MVIC of the QL (P=0.07). This consistent pattern across both muscles reinforces that WCKCe and WOKCe provide comparable benefits for enhancing lumbo-pelvic stabilizer strength, offering clinicians flexibility in exercise selection.
The underlying mechanisms for strength improvement in both muscles may involve similar neuromuscular adaptations, as both exercise types engage overlapping muscle groups and movement patterns [26, 29, 79, 103]. The comparative analysis of WCKCe and WOKCe reveals important implications for rehabilitation practices. Both exercise modalities leverage the unique properties of water to enhance muscle strength while minimizing the risk of injury associated with traditional land-based exercises [32, 33, 70]. Moreover, the findings suggest that clinicians can confidently implement either WCKCe or WOKCe in rehabilitation programs, depending on individual patient needs and preferences. For instance, WCKCe may be more suitable for patients requiring stability and support [44, 49, 50, 56, 108], while WOKCe could be advantageous for those aiming to enhance functional mobility and strength through a broader range of motion [53, 58]. The implications of these findings extend beyond immediate muscle strength improvements. Enhanced strength in the GMed and QL muscles is associated with improved functional outcomes, including better balance, stability, and overall physical performance. These factors are critical for athletes returning to sport and for individuals seeking to maintain an active lifestyle post-rehabilitation. The combination of TRB with hydrodynamic loading is particularly effective. Clinicians may freely choose between WCKCe and WOKCe for improving GMed and QL strength, as both yield comparable results. This provides flexibility to tailor programs to individual patient preferences and functional goals. This approach is especially beneficial for patients requiring low-impact training, such as those with LBP, hip pathologies, or during post-operative rehabilitation. Aquatic exercise offers an effective, flexible, and joint-protective approach to enhancing lumbo-pelvic stability and function.
This study has several limitations that should be addressed in future research. First, the long-term efficacy of both WCKCe and WOKCe on maintained strength improvements and functional outcomes remains unexplored. Second, the underlying neuromuscular adaptations, such as changes in motor unit recruitment patterns and muscle activation timing were not investigated. Additionally, the impact of these interventions on quality-of-life measures across diverse clinical populations warrants examination. Future studies should also establish optimal rehabilitation parameters by examining dose-response relationships through varied exercise intensities, durations, and frequencies. These investigations would substantiate the implementation of aquatic exercises as a primary strengthening modality rather than solely an initial rehabilitation approach.
Conclusion
Our study highlights the effectiveness of an 8-week aquatic exercise program in strengthening core muscles among men with CNSLBP. For clinicians, this underscores the importance of integrating aquatic therapy into rehabilitation strategies to enhance patient outcomes, including pain reduction and improved functional mobility. It is crucial for healthcare providers to tailor these interventions to individual patient needs and consider the study’s limitations when applying the findings. Future investigations should focus on the long-term effects and broader applicability of aquatic exercises in diverse patient populations to optimize low back pain management. Clinicians can select WCKCe or WOKCe considering patient mobility and preference without compromising strength gains.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee for Human Research at Bu-Ali Sina University, Hamadan, Iran (Code: IR.BASU.REC.1402.011). This study was registered by the Iranian Registry of Clinical Trials (IRCT) (Code: IRCT.20190129042534N1). Before experimental procedures began, all the participants reviewed and voluntarily signed an informed written consent form.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study design, and writing: Ali Yalfani; Data interpretation: Hossien Ashoury; Data acquisition, and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all participants in this study.
References
- Abadi FH, Choo LA, Elumalai G, Sankaravel M, Razli AI. Does aquatic exercise improve quality of life in obese low-back pain population? Int J Physiother. 2019; 6(4):128-33. [DOI:10.15621/ijphy/2019/v6i4/185415]
- Andias R, Silva AG. A systematic review with meta-analysis on functional changes associated with neck pain in adolescents. Musculoskeletal Care. 2019; 17(1):23-36. [DOI:10.1002/msc.1377] [PMID]
- Baena-Beato PÁ, Artero EG, Arroyo-Morales M, Robles-Fuentes A, Gatto-Cardia MC, Delgado-Fernández M. Aquatic therapy improves pain, disability, quality of life, body composition and fitness in sedentary adults with chronic low back pain. A controlled clinical trial. Clin Rehabil. 2014; 28(4):350-60. [DOI:10.1177/0269215513504943] [PMID]
- Bansal S, Katzman WB, Giangregorio LM. Exercise for improving age-related hyperkyphotic posture: A systematic review. Arch Phys Med Rehabil. 2014; 95(1):129-40. [DOI:10.1016/j.apmr.2013.06.022] [PMID]
- Bokaee F, Rezasoltani A, Manshadi FD, Naimi SS. Ultrasound echo intensity of cervical muscles in women with and without forward head posture. Cranio. 2022; 40(3):232-8. [DOI:10.1080/08869634.2020.1750806] [PMID]
- Carvalho RG, Silva MF, Dias JM, Olkoski MM, Bela LFD, Pelegrinelli AR, et al. Effectiveness of additional deep-water running for disability, lumbar pain intensity, and functional capacity in patients with chronic low back pain: A randomised controlled trial with 3-month follow-up. Musculoskelet Sci Pract. 2020; 49:102195. [DOI:10.1016/j.msksp.2020.102195] [PMID]
- Diab AA. The role of forward head correction in management of adolescent idiopathic scoliotic patients: A randomized controlled trial. Clin Rehabil. 2012; 26(12):1123-32. [DOI:10.1177/0269215512447085] [PMID]
- Fathollahnejad K, Letafatkar A, Hadadnezhad M. The effect of manual therapy and stabilizing exercises on forward head and rounded shoulder postures: A six-week intervention with a one-month follow-up study. BMC Musculoskelet Disord. 2019; 20. [DOI:10.1186/s12891-019-2438-y] [PMID]
- Meldrum D, Cahalane E, Keogan F, Hardiman O. Maximum voluntary isometric contraction: Investigation of reliability and learning effect. Amyotroph Lateral Scler Other Motor Neuron Disord. 2003; 4(1):36-44. [DOI:10.1080/14660820310006715] [PMID]
- Norcross MF, Blackburn JT, Goerger BM. Reliability and interpretation of single leg stance and maximum voluntary isometric contraction methods of electromyography normalization. J Electromyogr Kinesiol. 2010; 20(3):420-5. [DOI:10.1016/j.jelekin.2009.08.003] [PMID]
- Rutherford DJ, Hubley-Kozey CL, Stanish WD. Maximal voluntary isometric contraction exercises: a methodological investigation in moderate knee osteoarthritis. J Electromyogr Kinesiol. 2011; 21(1):154-60. [DOI:10.1016/j.jelekin.2010.09.004] [PMID]
- Peltonen H, Walker S, Lähitie A, Häkkinen K, Avela J. Isometric parameters in the monitoring of maximal strength, power, and hypertrophic resistance-training. Appl Physiol Nutr Metab. 2018; 43(2):145-53. [DOI:10.1139/apnm-2017-0310] [PMID]
- Hallgren RC, Pierce SJ, Sharma DB, Rowan JJ. Forward head posture and activation of rectus capitis posterior muscles. J Am Osteopath Assoc. 2017; 117(1):24-31. [DOI:10.7556/jaoa.2017.004] [PMID]
- Dankaerts W, O’Sullivan PB, Burnett AF, Straker LM, Danneels LA. Reliability of EMG measurements for trunk muscles during maximal and sub-maximal voluntary isometric contractions in healthy controls and CLBP patients. J Electromyogr Kinesiol. 2004; 14(3):333-42. [DOI:10.1016/j.jelekin.2003.07.001] [PMID]
- Worrell TW, Karst G, Adamczyk D, Moore R, Stanley C, Steimel B, et al. Influence of joint position on electromyographic and torque generation during maximal voluntary isometric contractions of the hamstrings and gluteus maximus muscles. J Orthop Sports Phys Ther. 2001; 31(12):730-40. [DOI:10.2519/jospt.2001.31.12.730] [PMID]
- Lee H, Hübscher M, Moseley GL, Kamper SJ, Traeger AC, Mansell G, et al. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain. 2015; 156(6):988-97. [DOI:10.1097/j.pain.0000000000000146] [PMID]
- Sahrmann S, Azevedo DC, Van Dillen L. Diagnosis and treatment of movement system impairment syndromes. Braz J Phys Ther. 2017; 21(6):391-9. [DOI:10.1016/j.bjpt.2017.08.001] [PMID]
- Ghaedi E, Tabatabaei H. [Comparison of eight weeks opened and closed chain exercises on strength and range of motion in female with chronic non-specific low back pain: A pilot study (Persian)]. J Community Health. 2022; 9(5):1-9. [DOI:10.22037/ch.v9i5.31520]
- McGill S. Low back disorders: Evidence-based prevention and rehabilitation. Champaign: Human Kinetics; 2025. [Link]
- McGill SM, Grenier S, Kavcic N, Cholewicki J. Coordination of muscle activity to assure stability of the lumbar spine. J Electromyogr Kinesiol. 2003; 13(4):353-9. [DOI:10.1016/S1050-6411(03)00043-9] [PMID]
- Nascimento MB, Vilarinho LG, Lobato DFM, Dionisio VC. Role of gluteus maximus and medius activation in the lower limb biomechanical control during functional single-leg tasks: A systematic review. Knee. 2023; 43:163-75. [DOI:10.1016/j.knee.2023.05.005] [PMID]
- Soomro RR, Karimi H, Gilani SA. Comparative efficacy of quadratus lumborum muscle energy technique with gluteus medius strengthening versus gluteus medius strengthening alone in sacroiliac joint dysfunction: A randomized controlled trial. Diagnostics. 2024; 14(21):2413. [DOI:10.3390/diagnostics14212413] [PMID]
- McGill S, Juker D, Kropf P. Appropriately placed surface EMG electrodes reflect deep muscle activity (psoas, quadratus lumborum, abdominal wall) in the lumbar spine. J Biomech. 1996; 29(11):1503-7. [DOI:10.1016/0021-9290(96)84547-7] [PMID]
- Baik SM, Cynn HS, Yi CH, Lee JH, Choi JH, Lee KE. Effect of side-sling plank exercise on trunk and hip muscle activation in subjects with gluteus medius weakness. J Back Musculoskelet Rehabil. 2022; 35(4):849-57. [DOI:10.3233/BMR-210061] [PMID]
- Cooper NA, Scavo KM, Strickland KJ, Tipayamongkol N, Nicholson JD, Bewyer DC, et al. Prevalence of gluteus medius weakness in people with chronic low back pain compared to healthy controls. Eur Spine J. 2016; 25:1258-65. [DOI:10.1007/s00586-015-4027-6] [PMID]
- Martinez-Merinero P, Nunez-Nagy S, Achalandabaso-Ochoa A, Fernandez-Matias R, Pecos-Martin D, Gallego-Izquierdo T. Relationship between forward head posture and tissue mechanosensitivity: A cross-sectional study. J Clin Med. 2020; 9(3). [DOI:10.3390/jcm9030634] [PMID]
- Lee JH, Cynn HS, Kwon OY, Yi CH, Yoon TL, Choi WJ, et al. Different hip rotations influence hip abductor muscles activity during isometric side-lying hip abduction in subjects with gluteus medius weakness. J Electromyogr Kinesiol. 2014; 24(2):318-24. [DOI:10.1016/j.jelekin.2014.01.008] [PMID]
- Ashoury H, Yalfani A. The effectiveness of exercise programs on the quadratus lumborum muscle in patients with chronic non-specific low back pain: A systematic review. Feyz Med Sci J. 2024; 28(1):110-22. [Link]
- Nelson-Wong E, Gregory DE, Winter DA, Callaghan JP. Gluteus medius muscle activation patterns as a predictor of low back pain during standing. Clin Biomech. 2008; 23(5):545-53. [DOI:10.1016/j.clinbiomech.2008.01.002] [PMID]
- Izzo R, Guarnieri G, Guglielmi G, Muto M. Biomechanics of the spine. Part I: Spinal stability. Eur J Radiol. 2013; 82(1):118-26. [DOI:10.1016/j.ejrad.2012.07.024] [PMID]
- Kell RT, Asmundson GJ. A comparison of two forms of periodized exercise rehabilitation programs in the management of chronic nonspecific low-back pain. J Strength Cond Res. 2009; 23(2):513-23. [DOI:10.1519/JSC.0b013e3181918a6e] [PMID]
- Cuesta-Vargas AI, García-Romero JC, Arroyo-Morales M, Diego-Acosta ÁM, Daly DJ. Exercise, manual therapy, and education with or without high-intensity deep-water running for nonspecific chronic low back pain: A pragmatic randomized controlled trial. Am J Phys Med Rehabil. 2011; 90(7):526-38. [DOI:10.1097/PHM.0b013e31821a71d0] [PMID]
- Psycharakis SG, Coleman SG, Linton L, Kaliarntas K, Valentin S. Muscle activity during aquatic and land exercises in people with and without low back pain. Phys Ther. 2019; 99(3):297-310. [DOI:10.1093/ptj/pzy150] [PMID]
- Tambuyzer E, Vandendriessche B, Austin CP, Brooks PJ, Larsson K, Miller Needleman KI, et al. Therapies for rare diseases: Therapeutic modalities, progress and challenges ahead. Nat Rev Drug Discov. 2020; 19(2):93-111. [DOI:10.1038/s41573-019-0049-9] [PMID]
- Beason KR, Gilbert J. Benefits of deep water exercise for ambulatory impaired adults. Palaestra. 1995; 11(4):22-8. [Link]
- Bergamin M, Zanuso S, Alvar BA, Ermolao A, Zaccaria M. Is water-based exercise training sufficient to improve physical fitness in the elderly? A systematic review of the evidence. Eur Rev Aging Phys Act. 2012; 9:129-41. [DOI:10.1007/s11556-012-0097-1]
- Cantarero-Villanueva I, Fernández-Lao C, Cuesta-Vargas AI, Del Moral-Avila R, Fernández-de-Las-Peñas C, Arroyo-Morales M. The effectiveness of a deep water aquatic exercise program in cancer-related fatigue in breast cancer survivors: A randomized controlled trial. Arch Phys Med Rehabil. 2013; 94(2):221-30. [DOI:10.1016/j.apmr.2012.09.008] [PMID]
- Goldstein E, Shoval E, Koren-Morag N. The effect of an exercise program in water on pain level and functional status in chronic nonspecific low back pain patients: A single-blind randomised controlled trial. J Nov Physiother Phys Rehabil. 2020; 7(2):049-56. [DOI:10.17352/2455-5487.000079]
- Kanitz AC, Machado B, Rodrigues D, Zambelli G, Ivaniski A, Carvalho N, et al. Deep-water running training at moderate intensity and high intensity improves pain, disability, and quality of life in patients with chronic low back pain: A randomized clinical trial. Arch Med Deporte. 2021; 38(1):28-35. [DOI:10.18176/archmeddeporte.00023]
- Kwok MM, Ng SS, Myers J, So BC. Aquatic high-intensity interval deep water running influence on cardiometabolic health and cognitive psychological responses in women. Med Sci Sports Exerc. 2024; 56(11):2203-10. [DOI:10.1249/MSS.0000000000003500] [PMID]
- Layne M. Water exercise. Champaign: Human Kinetics; 2015. [Link]
- Reilly T, Dowzer CN, Cable N. The physiology of deep-water running. J Sports Sci. 2003; 21(12):959-72. [DOI:10.1080/02640410310001641368] [PMID]
- Almansoof HS, Nuhmani S, Muaidi Q. Role of kinetic chain in sports performance and injury risk: A narrative review. J Med Life. 2023; 16(11):1591. [DOI:10.25122/jml-2023-0087] [PMID]
- Ashoury H, Yalfani A, Arjipour M. Assessing the impact of closed and open kinetic chain hydrotherapy on vertical ground reaction force, rate of loading, lumbo-pelvic stability, pain intensity, and kinesiophobia in men with non-specific chronic low back pain: A randomized clinical trial. J Rehabil Sci Res. 2025; 12(3):43-54. [DOI:10.30476/jrsr.2024.101742.1468]
- Bae W, Kim C. The effect of closed kinetic and open kinetic exercise on thickness of low back stabilization exercise using an ultrasonography imaging. J Korean Soc Integr Med. 2013; 1(2):67-80. [DOI:10.15268/ksim.2013.1.2.067]
- Brolinson PG, Rogers M, Edison J. Functional and kinetic chain evaluation of the hip and pelvis. Hip Pelvis Sports Med Prim Care. 2016; 37-64. [DOI:10.1007/978-3-319-42788-1_3]
- Fatollahi A, Barghamadi M, Darvishani MA. Effect of hydrotherapy on muscle activities and running kinetics in adult males with pronated foot: A randomized clinical trial. Pamukkale J Sport Sci. 2023; 14(3):297-313. [DOI:10.54141/psbd.1350754]
- Irish SE, Millward AJ, Wride J, Haas BM, Shum GL. The effect of closed-kinetic chain exercises and open-kinetic chain exercise on the muscle activity of vastus medialis oblique and vastus lateralis. J Strength Cond Res. 2010; 24(5):1256-62. [DOI:10.1519/JSC.0b013e3181cf749f] [PMID]
- Kwon YJ, Park SJ, Jefferson J, Kim K. The effect of open and closed kinetic chain exercises on dynamic balance ability of normal healthy adults. J Phys Ther Sci. 2013; 25(6):671-4. [DOI:10.1589/jpts.25.671] [PMID]
- Lephart SM, Henry TJ. The physiological basis for open and closed kinetic chain rehabilitation for the upper extremity. J Sport Rehabil. 1996; 5(1):71-87. [DOI:10.1123/jsr.5.1.71]
- Brody LT, Geigle PR, Geigle P. Aquatic exercise for rehabilitation and training. Human Kinetics; 2009. [DOI:10.5040/9781718210691]
- Lust KR. The effects of a six-week open kinetic chain/closed kinetic chain and open kinetic chain/closed kinetic chain/core stability strengthening program in baseball [MA thesis]. Virginia: West Virginia University; 2007. [Link]
- Sciascia A, Cromwell R. Kinetic chain rehabilitation: A theoretical framework. Rehabil Res Pract. 2012; 2012(1):853037. [DOI:10.1155/2012/853037] [PMID]
- Szczygiel E, Fudacz N, Golec J, Golec E. The impact of the position of the head on the functioning of the human body: A systematic review. Int J Occup Med Environ Health. 2020; 33(5):559-68. [DOI:10.13075/ijomeh.1896.01585] [PMID]
- Takındı EN, Çil ET. The effects of thoracic mobility versus lumbopelvic stabilization exercises on lower extremity flexibility, dynamic balance and proprioception in patients with chronic ankle instability. Isokinet Exerc Sci. 2024; 32(3):225-38. [DOI:10.3233/IES-230093]
- Tang SF, Chen CK, Hsu R, Chou SW, Hong WH, Lew HL. Vastus medialis obliquus and vastus lateralis activity in open and closed kinetic chain exercises in patients with patellofemoral pain syndrome: An electromyographic study. Arch Phys Med Rehabil. 2001; 82(10):1441-5. [DOI:10.1053/apmr.2001.26252] [PMID]
- Ashoury H, Yalfani A, Arjipour M. The effects of open/closed kinetic chain exercises in water on the electrical activity of selected lumbar muscles, lumbopelvic control, ground reaction force and psychological factors in men with chronic non-specific low back pain: A study protocol for a randomized clinical trial. J Bodyw Mov Ther 2024; 40:2147-54. [DOI:10.1016/j.jbmt.2024.10.065] [PMID]
- Ashoury H, Yalfani A, Arjipour M. The influence of hydrotherapy kinetic chain exercises on plantar pressure variables, pain, disability and kinesiophobia in men with non-specific chronic low back pain: An experiment with randomized clinical trial. Phys Treat Specif Phys Ther J. 2025; 15(3):0-. [DOI:10.32598/ptj.15.3.609.1]
- Ma J, Zhang T, He Y, Li X, Chen H, Zhao Q. Effect of aquatic physical therapy on chronic low back pain: A systematic review and meta-analysis. BMC Musculoskelet Disord. 2022; 23(1):1050. [DOI:10.1186/s12891-022-05981-8] [PMID]
- Psycharakis SG, Coleman SG, Linton L, Valentin S. The water study: Which aquatic exercises increase muscle activity and limit pain for people with low back pain? Physiotherapy. 2022; 116:108-18. [DOI:10.1016/j.physio.2022.03.003] [PMID]
- Shi Z, Zhou H, Lu L, Pan B, Wei Z, Yao X, et al. Aquatic exercises in the treatment of low back pain: A systematic review of the literature and meta-analysis of eight studies. Am J Phys Med Rehabil. 2018; 97(2):116-22. [DOI:10.1097/PHM.0000000000000801] [PMID]
- Aali S, Rezazadeh F, Imani F, Sefidekhan MN, Badicu G, Poli L, et al. Effects of exercise-based rehabilitation on lumbar degenerative disc disease: A systematic review. Healthcare. 2025. [DOI:10.3390/healthcare13151938] [PMID]
- Deodato M, Guolo F, Monticco A, Fornari M, Manganotti P, Granato A. Osteopathic manipulative therapy in patients with chronic tension-type headache: A pilot study. J Am Osteopath Assoc. 2019; 119(10):682-7. [DOI:10.7556/jaoa.2019.093] [PMID]
- Saghaei M. Random allocation software for parallel group randomized trials. BMC Med Res Methodol. 2004; 4:1-6. [DOI:10.1186/1471-2288-4-26] [PMID]
- Boutron I, Estellat C, Guittet L, Dechartres A, Sackett DL, Hróbjartsson A, et al. Methods of blinding in reports of randomized controlled trials assessing pharmacologic treatments: A systematic review. Plos Med. 2006; 3(10):e425. [DOI:10.1371/journal.pmed.0030425] [PMID]
- Hróbjartsson A, Thomsen ASS, Emanuelsson F, Tendal B, Hilden J, Boutron I, et al. Observer bias in randomised clinical trials with binary outcomes: Systematic review of trials with both blinded and non-blinded outcome assessors. BMJ. 2012; 344. [DOI:10.1136/bmj.e1119] [PMID]
- Altman DG, Schulz KF, Moher D, Egger M, Davidoff F, Elbourne D, et al. The revised CONSORT statement for reporting randomized trials: Explanation and elaboration. Ann Intern Med. 2001; 134(8):663-94. [DOI:10.7326/0003-4819-134-8-200104170-00012] [PMID]
- Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, Group* C. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann Intern Med. 2008; 148(4):295-309. [DOI:10.7326/0003-4819-148-4-200802190-00008] [PMID]
- Hopewell S, Chan AW, Collins GS, Hróbjartsson A, Moher D, Schulz KF, et al. CONSORT 2025 explanation and elaboration: Updated guideline for reporting randomised trials. BMJ. 2025; 389:e081124. [PMID]
- Becker BE. Aquatic therapy: Scientific foundations and clinical rehabilitation applications. PM R. 2009; 1(9):859-72. [DOI:10.1016/j.pmrj.2009.05.017] [PMID]
- Cole AJ, Becker BE. Comprehensive aquatic therapy. Oxford: Butterworth-Heinemann; 2004. [Link]
- Lee J, Choi E, Kim M, Yoon Y, Choi S. PreventFHP: Detection and warning system for forward head posture. In: Omalley M, Choi S, Kuchenbecker KJ, editors. 2014 Ieee Haptics Symposium. IEEE haptics symposium. 2014; 295-8. [DOI:10.1109/HAPTICS.2014.6775470]
- Dayanır IO, Birinci T, Kaya Mutlu E, Akcetin MA, Akdemir AO. Comparison of three manual therapy techniques as trigger point therapy for chronic nonspecific low back pain: A randomized controlled pilot trial. J Altern Complement Med. 2020; 26(4):291-9. [DOI:10.1089/acm.2019.0435] [PMID]
- Buckthorpe M, Pirotti E, Della Villa F. Benefits and use of aquatic therapy during rehabilitation after ACL reconstruction-a clinical commentary. Int J Sports Phys Ther. 2019; 14(6):978. [DOI:10.26603/ijspt20190978] [PMID]
- Heidari F, Mohammad Rahimi N, Aminzadeh R. Aquatic exercise impact on pain intensity, disability and quality of life in adults with low back pain: A systematic review and meta-analysis. Biol Res Nurs. 2023; 25(4):527-41. [DOI:10.1177/10998004231162327] [PMID]
- Rezai V, Mahdavi-Nejad R, Zolaktaf V. Comparing the effects of different types of aquatic walking on endurance and electrical activities of spine extensor muscles in men with nonspecific chronic back pain. Int J Prev Med. 2020; 11(1):168. [DOI:10.4103/ijpvm.IJPVM_403_19] [PMID]
- Ahmadnezhad L, Yalfani A, Gholami-Borujeni B. Increasing activity and co-contraction of local muscles in the core region and lumbopelvic motor control through immediate respiratory muscle training: A double-blind randomized controlled trial. J Kerman Univ Med Sci. 2022; 29(1):39-49.[Link]
- Vulfsons S, Chervonenko S, Haddad M, Weisman M, Lavi N, Dar G. Decreased amplitude of surface electromyo-graphic recordings of muscle activation along the posterior myofascial kinematic chain in subjects with chronic nonspecific low back pain compared to healthy subjects. J Back Musculoskelet Rehabil. 2018; 31(4):785-93. [DOI:10.3233/BMR-160627] [PMID]
- Muyor JM, Martín-Fuentes I, Rodríguez-Ridao D, Antequera-Vique JA. Electromyographic activity in the gluteus medius, gluteus maximus, biceps femoris, vastus lateralis, vastus medialis and rectus femoris during the Monopodal Squat, Forward Lunge and Lateral Step-Up exercises. Plos One. 2020; 15(4):e0230841. [DOI:10.1371/journal.pone.0230841] [PMID]
- Andersson EA. EMG and strength in trunk and hip muscles [PhD dissertation]. Solna: Karolinska Institutet; 1997. [Link]
- Ahn WC, Min KB, Kim MK. Comparison of core muscle activation at different hip angles during core exercises based on dynamic neuromuscular stabilization. Asian J Kinesiol. 2025; 27(1):45-52. [DOI:10.15758/ajk.2025.27.1.45]
- Andersson E, Oddsson L, Grundström H, Nilsson J, Thorstensson A. EMG activities of the quadratus lumborum and erector spinae muscles during flexion-relaxation and other motor tasks. Clin Biomech. 1996; 11(7):392-400. [DOI:10.1016/0268-0033(96)00033-2] [PMID]
- Meldrum D, Cahalane E, Conroy R, Fitzgerald D, Hardiman O. Maximum voluntary isometric contraction: Reference values and clinical application. Amyotroph Lateral Scler. 2007; 8(1):47-55. [DOI:10.1080/17482960601012491] [PMID]
- Ng JKF, Parnianpour M, Richardson CA, Kippers V. Functional roles of abdominal and back muscles during isometric axial rotation of the trunk. J Orthop Res. 2001; 19(3):463-71. [DOI:10.1016/S0736-0266(00)90027-5] [PMID]
- Gholami-Borujeni B, Yalfani A, Ahmadnezhad L. Eight-week inspiratory muscle training alters electromyography activity of the ankle muscles during overhead and single-leg squats: A randomized controlled trial. J Appl Biomech. 2020; 37(1):13-20. [DOI:10.1123/jab.2019-0315] [PMID]
- Golparian M, Anbarian M, Golparian A. Effects of trunk and foot positions on electromyographic activity and co-contraction of selected lower extremity muscles during leg-press resistance training. J Adv Sport Technol. 2021; 5(1):17-26. [Link]
- Richardson JT. Eta squared and partial eta squared as measures of effect size in educational research. Educ Res Rev. 2011; 6(2):135-47. [DOI:10.1016/j.edurev.2010.12.001]
- Wu A, March L, Zheng X, Huang J, Wang X, Zhao J, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann Transl Med. 2020; 8(6). [DOI:10.21037/atm.2020.02.175] [PMID]
- Soufivand P, Gandomi F, Assar S, Abbasi H, Salimi M, Ezati M, et al. The effect of a six-week aqua pilates and aqua stretch intervention on pain, function, and quality of life in patients affected by ankylosing spondylitis: A rater-blind randomized controlled trial. J Back Musculoskelet Rehabil. 2024. [Preprint]. [DOI:10.3233/BMR-230077]
- Hajouj E, Hadian MR, Mir SM, Talebian S, Ghazi S. Effects of innovative aquatic proprioceptive training on knee proprioception in athletes with anterior cruciate ligament reconstruction: A randomized controlled trial. Arch Bone Jt Surg. 2021; 9(5):519. [DOI:10.5812/ans.111430]
- Peng MS, Wang R, Wang YZ, Chen CC, Wang J, Liu XC, et al. Efficacy of therapeutic aquatic exercise vs physical therapy modalities for patients with chronic low back pain: A randomized clinical trial. JAMA Netw Open. 2022; 5(1):e2142069.[DOI:10.1001/jamanetworkopen.2021.42069] [PMID]
- Colado JC, Borreani S, Pinto SS, Tella V, Martin F, Flandez J, et al. Neuromuscular responses during aquatic resistance exercise with different devices and depths. J Strength Cond Res. 2013; 27(12):3384-90. [DOI:10.1519/JSC.0b013e3182915ebe] [PMID]
- Gillis GB, Blob RW. How muscles accommodate movement in different physical environments: Aquatic vs. terrestrial locomotion in vertebrates. Comp Biochem Physiol A Mol Integr Physiol. 2001; 131(1):61-75. [DOI:10.1016/S1095-6433(01)00466-4] [PMID]
- Wilk K, Joyner D. The use of aquatics in orthopedics and sports medicine rehabilitation and physical conditioning.Taylor & Francis; 2024. [DOI:10.4324/9781003526865]
- Kim E, Kim T, Kang H, Lee J, Childers MK. Aquatic versus land-based exercises as early functional rehabilitation for elite athletes with acute lower extremity ligament injury: A pilot study. PM R. 2010; 2(8):703-12. [DOI:10.1016/j.pmrj.2010.03.012] [PMID]
- Kim Y, Vakula MN, Waller B, Bressel E. A systematic review and meta-analysis comparing the effect of aquatic and land exercise on dynamic balance in older adults. BMC Geriatr. 2020; 20:1-14. [DOI:10.1186/s12877-020-01702-9] [PMID]
- Maleki B, Raisi Z. The effect of aquatic and land-based exercises on pain reduction, muscle strength and kinetic/kinematic variables in people with chronic low back pain: A review study. J Sport Biomech. 2018; 4(3):2-13. [DOI:10.32598/biomechanics.4.3.2]
- Hodges PW, Richardson CA. Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Arch Phys Med Rehabil. 1999; 80(9):1005-12. [DOI:10.1016/S0003-9993(99)90052-7] [PMID]
- Pires D, Cruz EB, Caeiro C. Aquatic exercise and pain neurophysiology education versus aquatic exercise alone for patients with chronic low back pain: A randomized controlled trial. Clin Rehabil. 2015; 29(6):538-47. [DOI:10.1177/0269215514549033] [PMID]
- Rafeeyan Z, Mostafa Musa F. The Effectiveness of aquatic exercises on pain and disability of the patients with chronic low back pain. Evid Based Care. 2014; 3(4):39-46. [DOI:10.22038/ebcj.2013.2055]
- Olkoski MM, Silva MF, Guenka LC, Pelegrinelli AR, Dela Bela LF, Dias JM, et al. Comparing the effects of aquatic exercises with or without high intensity on the functional status, muscular endurance, and performance of patients with chronic low back pain. J Sports Med Phys Fit. 2020; 61(5):699-706. [DOI:10.23736/S0022-4707.20.11265-9] [PMID]
- Cha SH, Kim SH, Baik SM, Cynn HS. The application of thera-band on non-weight bearing leg influence hip abductor activities during pelvic drop exercise in patients with gluteus medius weakness. Phys Ther Korea. 2023; 30(1):68-77. [DOI:10.12674/ptk.2023.30.1.68]
- Moore D, Semciw AI, Pizzari T. A systematic review and meta-analysis of common therapeutic exercises that generate highest muscle activity in the gluteus medius and gluteus minimus segments. Int J Sports Phys Ther. 2020; 15(6):856. [DOI:10.26603/ijspt20200856] [PMID]
- Thebuwanaarachchi S, Samarawickrama M, Dissanayake A, Gunawardena S, De Silva Y, Paris M, et al. Effectiveness of thera-band exercise program and electro-physiotherapy on abductor strength of the iliotibial band in athletes with iliotibial band syndrome. Sri Lanka Anat J. 2024; 7(2). [DOI:10.4038/slaj.v7i2.206]
- Youdas JW, Adams KE, Bertucci JE, Brooks KJ, Nelson MM, Hollman JH. Muscle activation levels of the gluteus maximus and medius during standing hip-joint-strengthening exercises using elastic-tubing resistance. J Sport Rehabil. 2014; 23(1):1-11. [PMID]
- Rosenstein B, Montpetit C, Vaillancourt N, Dover G, Khalini-Mahani N, Weiss C, et al. Effect of aquatic exercise versus standard care on paraspinal and gluteal muscles morphology in individuals with chronic low back pain: A randomized controlled trial protocol. BMC Musculoskelet Disord. 2023; 24(1):977. [DOI:10.1186/s12891-023-07034-0] [PMID]
- Bunton EE, Pitney WA, Cappaert TA, Kane AW. The role of limb torque, muscle action and proprioception during closed kinetic chain rehabilitation of the lower extremity. J Athl Train. 1993; 28(1):10. [Link]
- Öberg B, Good L, Kvist J. A comprehensive rehabilitation program with quadriceps strengthening in closed versus open kinetic chain in patients with anterior cruciate ligament deficiency: A randomized clinical trial evaluating dynamic tibial translation and muscle function. Am J Sports Med. 2008; 36(2):298-307. [DOI:10.1177/0363546507307867] [PMID]
- Ebert JR, Edwards PK, Fick DP, Janes GC. A systematic review of rehabilitation exercises to progressively load the gluteus medius. J Sport Rehabil. 2017; 26(5):418-36. [DOI:10.1123/jsr.2016-0088] [PMID]
- Stastny P, Tufano JJ, Golas A, Petr M. Strengthening the gluteus medius using various bodyweight and resistance exercises. Strength Cond J. 2016; 38(3):91-101. [DOI:10.1519/SSC.0000000000000221] [PMID]
- Yu W, An C, Kang H. Effects of resistance exercise using thera-band on balance of elderly adults: A randomized controlled trial. J Phys Ther Sci. 2013; 25(11):1471-3. [DOI:10.1589/jpts.25.1471] [PMID]
- Baik SM, Cynn HS, Kim SH. Understanding and exercise of gluteus medius weakness: A systematic review. PhysTher Korea. 2021; 28(1):27-35. [DOI:10.12674/ptk.2021.28.1.27]
- Yalfani A, Raeisi Z, Koumasian Z. Effects of eight-week water versus mat pilates on female patients with chronic nonspecific low back pain: Double-blind randomized clinical trial. J Bodyw Mov Ther. 2020; 24(4):70-5. [DOI:10.1016/j.jbmt.2020.06.002] [PMID]
- Ocampo JAR. The effects of the Brugger theraband method on gluteal muscle activation in patients with gluteal tendinopathy [PhD dissertation]. California: Azusa Pacific University; 2018. [Link]
Type of Study: Research Article |
Subject:
Spine surgery
Received: 2025/01/12 | Accepted: 2025/04/21 | Published: 2025/08/1
Received: 2025/01/12 | Accepted: 2025/04/21 | Published: 2025/08/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
