

Volume 12, Issue 4 (Autumn 2025)
JROS 2025, 12(4): 171-180 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nakahei Amroodi M, Tabrizian P, Mahdavifar M, Bahaeddini M, Karami M, Hashemipour B et al . Clinical Outcomes of Surgical Debridement and Intravenous Antibiotic Therapy in Patients With Postoperative Infection Following Open or Arthroscopic Rotator Cuff Repair. JROS 2025; 12 (4) :171-180
URL: http://jros.iums.ac.ir/article-1-2307-en.html
URL: http://jros.iums.ac.ir/article-1-2307-en.html
Morteza Nakahei Amroodi1 

 , Pouria Tabrizian1 , Mohammadmehdi Mahdavifar1 , Mohammadreza Bahaeddini1 , Mehdi Karami1 , Babak Hashemipour1 , Mojtaba Khajeh Alizadeh Attar1
, Pouria Tabrizian1 , Mohammadmehdi Mahdavifar1 , Mohammadreza Bahaeddini1 , Mehdi Karami1 , Babak Hashemipour1 , Mojtaba Khajeh Alizadeh Attar1
, Pouria Tabrizian1 , Mohammadmehdi Mahdavifar1 , Mohammadreza Bahaeddini1 , Mehdi Karami1 , Babak Hashemipour1 , Mojtaba Khajeh Alizadeh Attar1
1- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Rotator cuff tear, Open surgery, Secondary infection, C-reactive protein (CRP), Erythrocyte sedimentation rate (ESR), Intravenous antibiotics
Full-Text [PDF 613 kb]
(42 Downloads)
| Abstract (HTML) (190 Views)
Full-Text: (11 Views)
Introduction
Rotator cuff repair (RCR) is a commonly performed orthopaedic procedure for symptomatic rotator cuff tears, which are a frequent cause of shoulder pain and dysfunction worldwide [1]. Although operative repair generally achieves good clinical outcomes, postoperative complications can occur [2]. Deep infection is one of the most serious but relatively rare complications, with a reported incidence ranging between approximately 0.3% and 3.4% after rotator cuff surgery [3].
Deep infections after RCR may present with increasing shoulder pain, stiffness, swelling, local erythema, and systemic signs depending on severity. Because the glenohumeral joint is relatively deep and surrounded by soft tissue, clinical signs may be subtle, and definitive diagnosis often requires laboratory and microbiological evaluation. Elevated inflammatory markers, such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), are commonly used as surrogate markers of infection and treatment response. However, these markers are nonspecific and must be interpreted in conjunction with clinical findings [4-6].
The microbiological profile of postoperative shoulder infections includes various organisms. Traditional pathogens, such as Staphylococcus aureus and coagulase-negative staphylococci, have been reported. However, the anaerobic skin commensal Cutibacterium acnes (formerly Propionibacterium acnes) has emerged as a frequent isolate in deep shoulder infections following RCR, particularly in arthroscopic cases [3].
The management of deep infections after RCR typically involves a combination of surgical debridement, irrigation, drainage placement, and targeted antibiotic therapy. Prompt and aggressive treatment is crucial to eradicate the infection, prevent further soft tissue damage (including chondral destruction and muscle compromise), and improve functional outcomes. However, published literature is limited regarding comparative outcomes of open versus arthroscopic management, patterns of laboratory marker changes, and optimal antibiotic regimens in this specific clinical setting [3].
Given the potential for significant morbidity associated with infection after RCR and the relatively limited focused evidence, further investigation into clinical and laboratory outcomes following standardized treatment protocols is warranted [7]. Therefore, this study aimed to evaluate the effects of surgical debridement, prolonged drainage, and intravenous antibiotic therapy on ESR and CRP levels in patients with postoperative infection following open or arthroscopic RCR, and to characterize the microbiological profile of the infecting agents.
Methods
This retrospective cross-sectional study was conducted at Shafayahyaeian and Iranmehr Hospitals, two tertiary referral centers in Tehran Province, Iran. The study protocol was approved by the Ethics Committee of Iran University of Medical Sciences. All patients who presented between 2017 and 2024 with postoperative infection following surgical repair of a rotator cuff tear were considered for inclusion. Eligible patients were identified through review of hospital medical records. The inclusion criteria consisted of a history of rotator cuff tendon repair performed by either open surgery or arthroscopically, and a confirmed infection related to the prior RCR. Patients with incomplete or missing medical records were excluded from the study. A convenience sampling method was used, and all patients meeting the inclusion criteria during the study period were enrolled. Data were retrospectively collected through a review of medical records. The extracted variables included demographic characteristics (age and sex), comorbid conditions, such as diabetes mellitus and hypertension, type of primary RCR (open or arthroscopic), type and duration of intravenous antibiotic therapy, and microbiological findings based on culture results. Clinical evaluation of treatment success was performed by monitoring laboratory inflammatory markers, including ESR and CRP. These markers were recorded at three time points: prior to surgical intervention, one week after initiation of intravenous antibiotic therapy, and at hospital discharge. The type and duration of intravenous antibiotic therapy were also documented.
Statistical analysis
Statistical analyses were performed using the SPSS software, version 24 (IBM Corp., Armonk, NY, USA). Continuous variables were reported as Mean±SD, along with minimum and maximum values. A repeated-measures analysis was used to evaluate changes in ESR and CRP levels across the three time points (preoperative, one week after antibiotic initiation, and discharge). A P<0.05 was considered statistically significant. Patient confidentiality was strictly maintained, and all data were anonymized prior to analysis.
Surgical procedure
Following confirmation of infection, patients were transferred to the operating room for irrigation and debridement under general anesthesia in a semi-sitting position. The previous surgical incision was reopened. Granulation tissue located beneath the deltoid muscle and within the glenohumeral joint was identified and sampled for microbiological culture and pathological evaluation. All previously implanted suture materials were removed. Necrotic and infected tissues were thoroughly debrided, followed by extensive irrigation. The rotator cuff was repaired using nylon sutures. The long head of the biceps tendon was tenodesed. The coracoacromial ligament and deltoid muscle were repaired using nylon sutures. Two drains were inserted at the infection site—one intra-articular and one beneath the deltoid muscle. The skin was closed using nylon sutures, and the shoulder was immobilized with a sling. Drains were maintained for three weeks to facilitate continuous evacuation of infectious secretions. Intravenous antibiotic therapy was administered and adjusted according to culture results and continued until clinical improvement was achieved.
Results
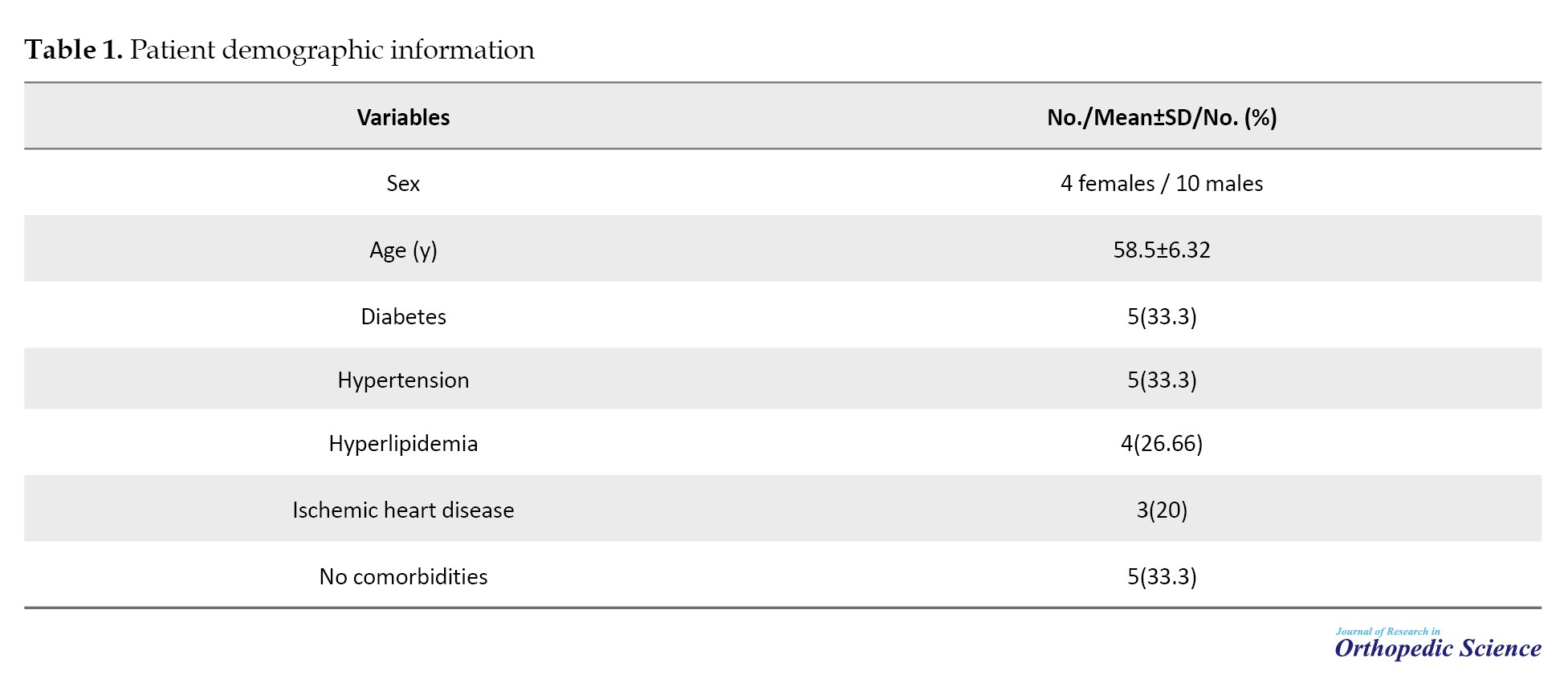
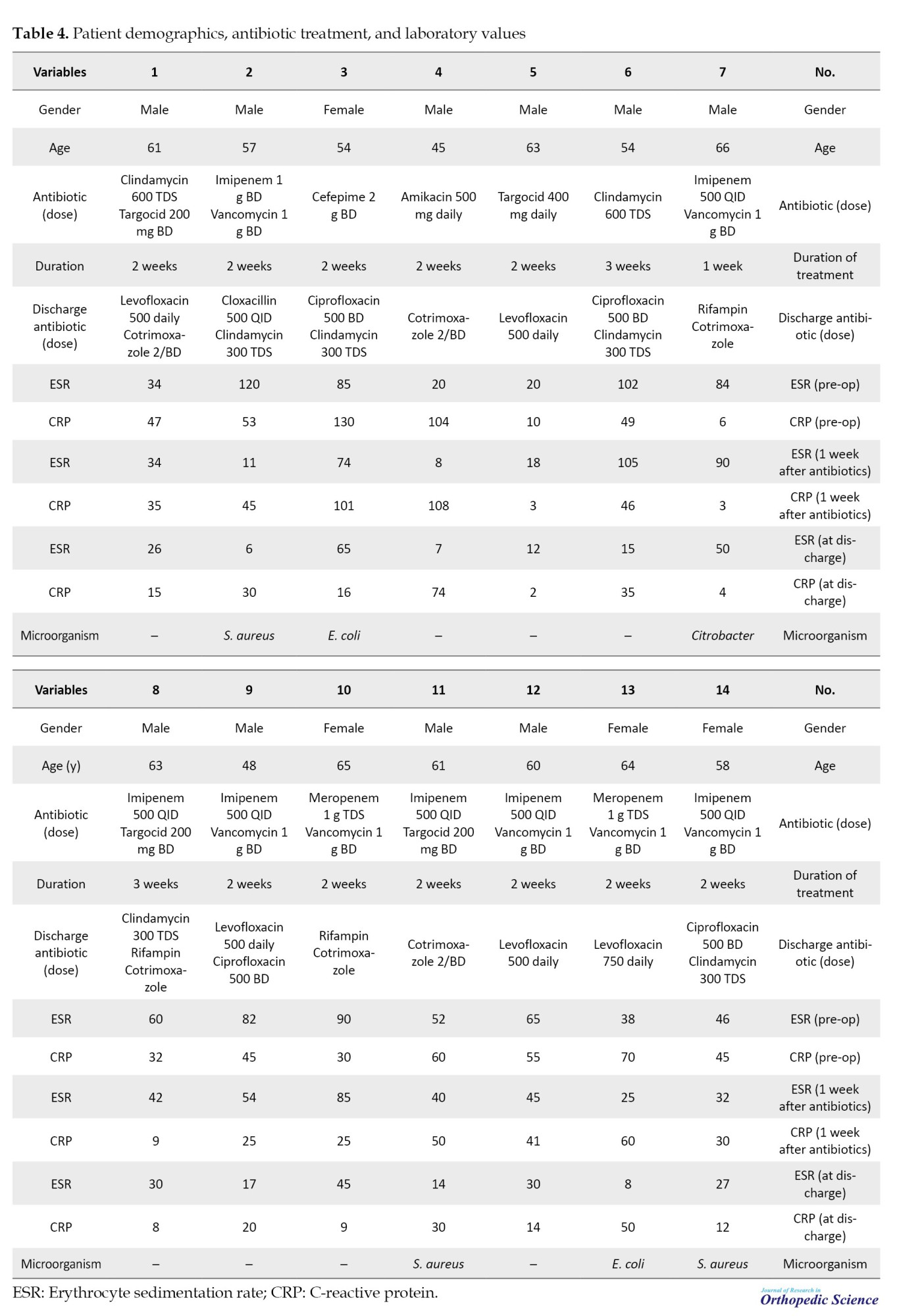
A total of 14 patients who underwent surgical intervention for postoperative infection following open RCR between 2017 and 2024 at Shafayahyaeian and Iranmehr hospitals were included in the study. The cohort consisted of 10 men (71.4%) and 4 women (28.6%) with a mean age of 58.5±6.32 years (range, 45–66 years).
Regarding baseline comorbidities, five patients (33.3%) had diabetes mellitus, five patients (33.3%) had hypertension, four patients (26.6%) had hyperlipidemia, and three patients (20%) had ischemic heart disease. Two patients had three comorbidities, four patients had two, and five patients (33.3%) had no documented underlying diseases (Table 1).
Microbiological findings
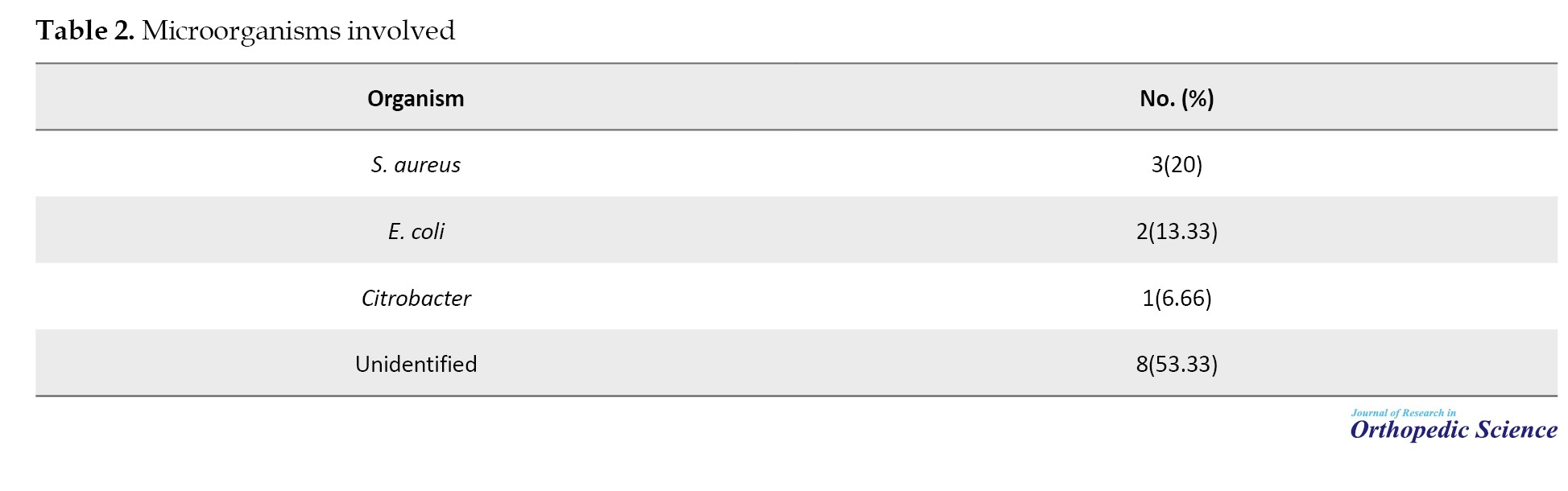
Microbiological culture results demonstrated that S. aureus was identified in three patients (20%), Escherichia coli in two patients (13.3%), and Citrobacter species in one patient (6.6%). In eight patients (53.3%), no specific organism was isolated from culture specimens (Table 2).
Antibiotic therapy
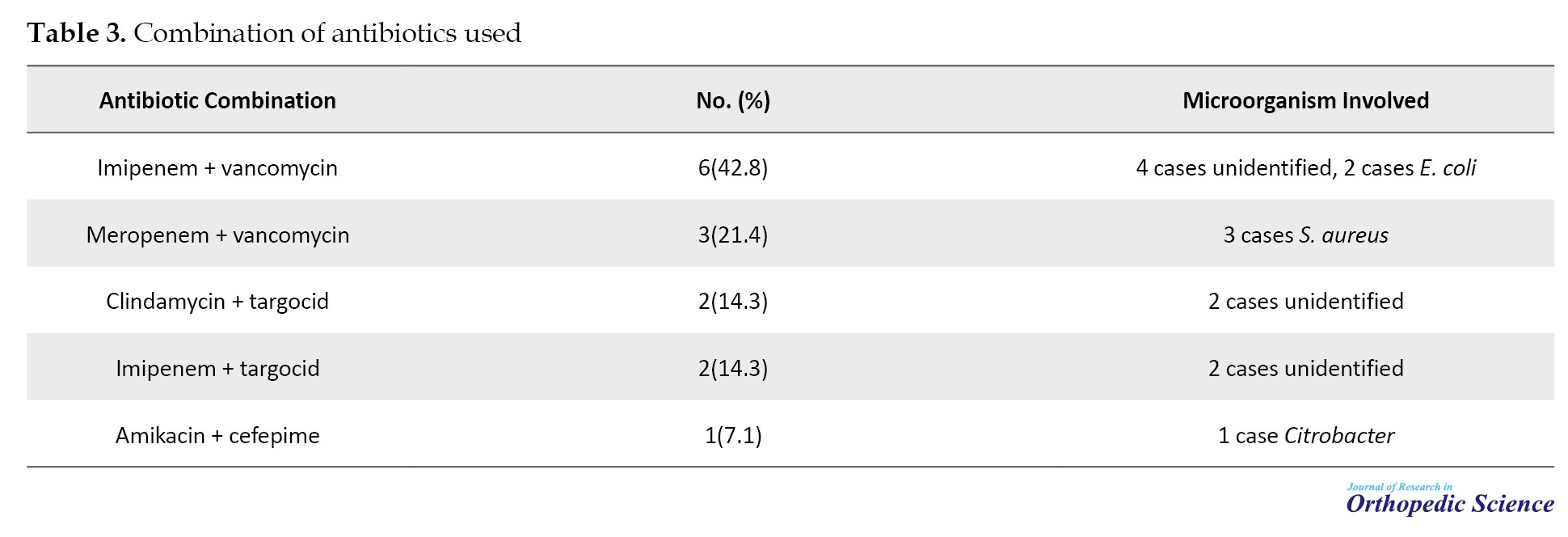
Following surgical debridement and drain placement, the most commonly administered antibiotic regimen was a combination of imipenem and vancomycin, which was used in six patients (42.8%). Other antibiotic combinations included meropenem plus vancomycin in three patients (21.4%), clindamycin plus teicoplanin (targocid) in two patients (14.3%), imipenem plus teicoplanin in two patients (14.3%), and amikacin plus cefepime in one patient (7.2%) (Table 3).
The mean duration of intravenous antibiotic therapy was approximately two weeks in the majority of patients, with extended treatment up to three weeks in selected cases. At discharge, patients were transitioned to oral antibiotic regimens tailored according to culture results and clinical response.
One patient required modification of the antibiotic regimen due to persistent elevation of inflammatory markers, necessitating the addition of meropenem and cotrimoxazole. In another case (patient 7), no drain was placed during the initial surgery. This patient demonstrated an increase in ESR and CRP one week after antibiotic initiation and subsequently underwent a second surgical intervention with drain placement. The antibiotic regimen was modified to linezolid and rifampin, with amikacin added four days later.
Laboratory outcomes
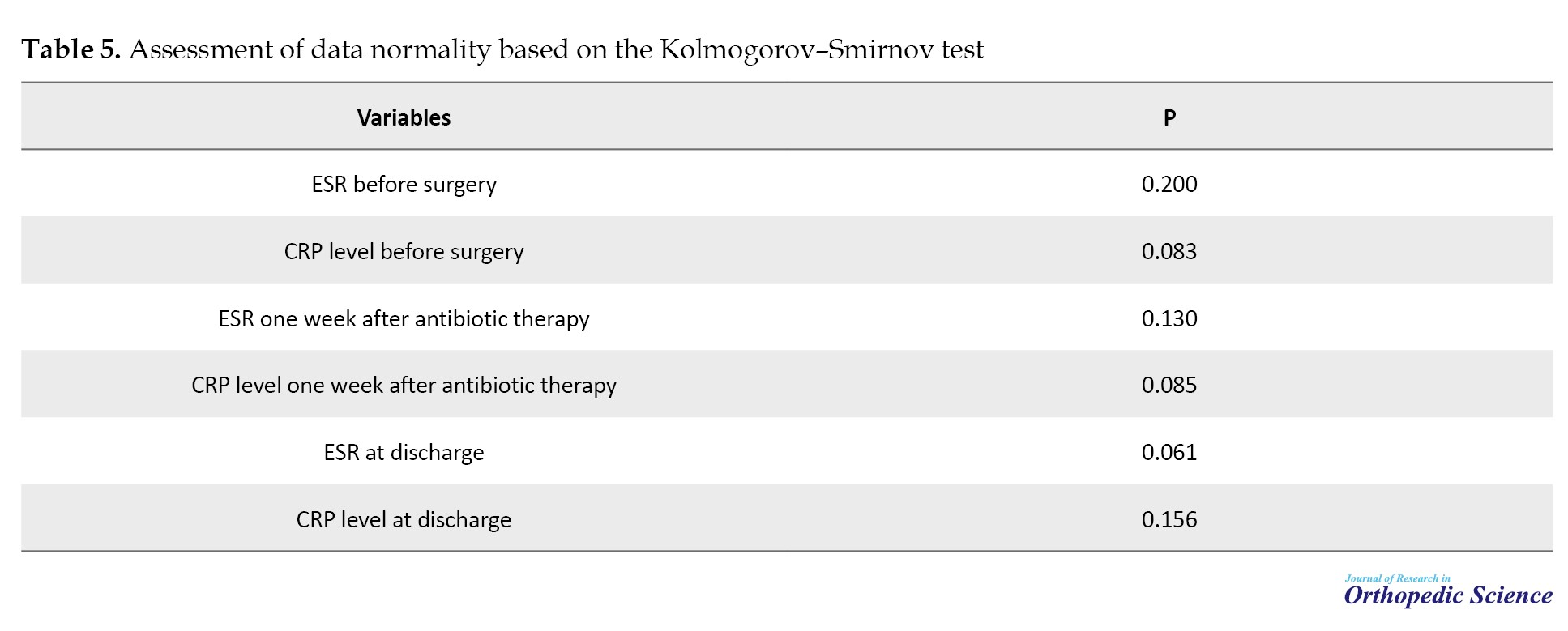
Normality testing using the Kolmogorov–Smirnov test demonstrated that ESR and CRP values at all measured time points followed a normal distribution (all P>0.05), allowing for parametric analysis (Tables 4, 5, and 6).
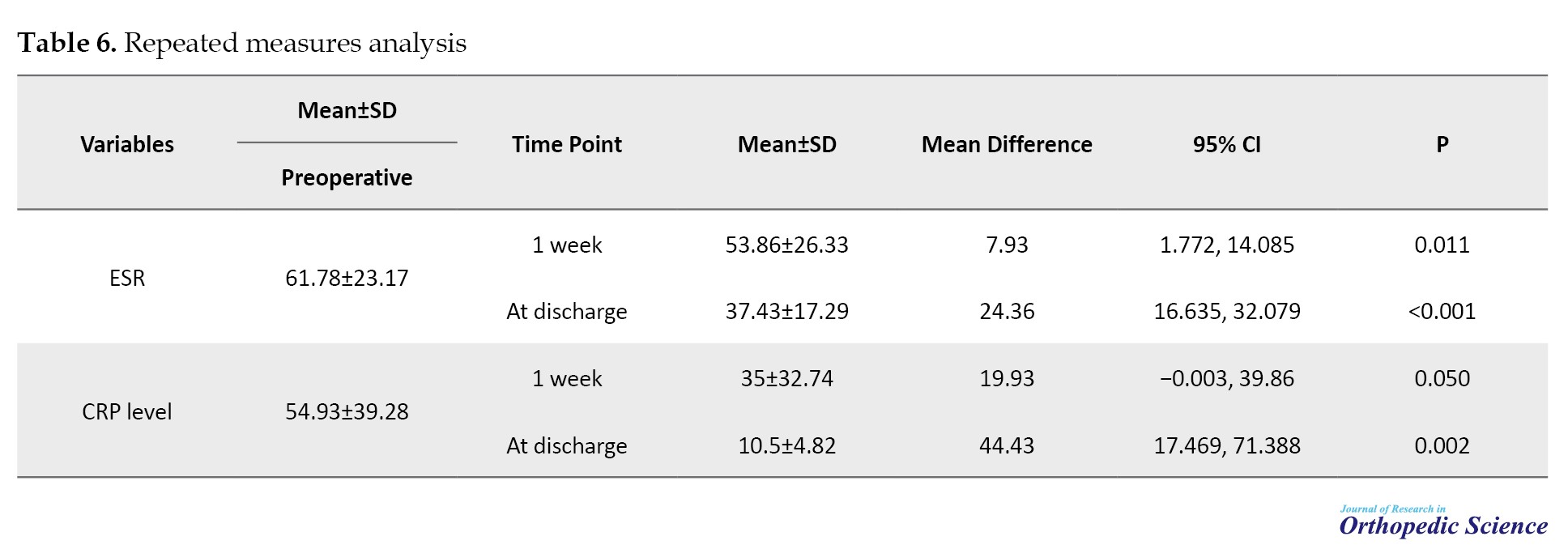
A repeated-measures analysis was performed to evaluate changes in inflammatory markers over time (preoperatively, one week after initiation of antibiotic therapy, and at discharge).
The mean preoperative ESR was 61.78±23.17 mm/h. One week after the initiation of antibiotic therapy, ESR decreased to 53.86±26.33 mm/h, representing a mean reduction of 7.93 mm/hour from baseline (95% confidence interval [CI], 1.77%, 14.08%; P=0.011). At discharge, ESR further decreased to 37.43±17.29 mm/h, corresponding to a mean reduction of 24.36 mm/h relative to baseline (95% CI, 16.63%, 32.07%; P<0.001).
The mean preoperative CRP level was 54.93±39.28 mg/L. One week after antibiotic initiation, CRP decreased to 35.74±32.74 mg/L; however, this reduction did not reach statistical significance compared with baseline (mean difference: 19.93 mg/L; 95% CI, −0.003%, 39.86%; P=0.050). At discharge, CRP significantly decreased to 10.5±4.82 mg/L, reflecting a mean reduction of 44.43 mg/L compared to preoperative values (95% CI, 17.46%, 71.38%; P=0.002).
Overall, ESR levels decreased significantly both one week after antibiotic therapy and at discharge, whereas CRP levels decreased significantly only at discharge.
Discussion
The results of the present study demonstrated that the combined use of drains and antibiotics for an average of two weeks effectively reduced CRP and ESR levels. The most common microorganism responsible for secondary infection was S. aureus. In contrast, the most frequently used antibiotic regimen for infection control was a combination of imipenem and vancomycin, administered to approximately half of the patients.
Kwon et al. [2] investigated 14 patients with early-onset infections (<6 weeks) and reported that the most frequent clinical manifestations included wound discharge and local erythema, while white blood cell counts often remained within normal ranges. In that study, ESR was elevated in all patients, and CRP levels were abnormal in the evaluated cases. The authors emphasized that CRP decreases more rapidly than ESR and is therefore more useful for early diagnosis, whereas ESR decreases more slowly and is better suited for long-term monitoring [2]. Our findings align with this pattern, demonstrating a faster reduction in CRP at discharge and a more sustained decrease in ESR throughout treatment.
Similarly, a systematic review by Smith et al. [8] encompassing over 10,000 RCRs found that CRP was elevated in 83% of patients with infection, whereas ESR was elevated in only 25%. The study concluded that CRP is a more sensitive marker for detecting acute infections, while ESR may remain normal in many patients. A comparison of our data with that of this review suggests that using both markers concurrently can improve the accuracy of infection diagnosis and treatment monitoring.
Shi et al. [9] also highlighted the importance of combining traditional methods (ESR, CRP, cultures) with advanced techniques, such as PCR and sonication, for more accurate diagnosis of shoulder infections. This study demonstrated that CRP is particularly valuable for evaluating the initial response to treatment, whereas ESR is more suitable for long-term monitoring. Our findings corroborate this conclusion, indicating that a decrease in CRP at discharge can be considered a marker of successful treatment.
In contrast, Mirzayan et al. [10] evaluated patients with chronic infections (mean 9.7 months post-surgery) and reported that these patients typically presented with elevated ESR and normal white blood cell counts. Infection control often required multiple debridements, sometimes including muscle flaps. Although the infection was eventually controlled, many patients experienced significant functional limitations. These findings underscore the importance of early diagnosis and intervention, as delays may lead to soft-tissue and bone destruction and poor functional outcomes.
Overall, our findings confirm that CRP is more suitable for early diagnosis and rapid assessment of treatment response, whereas ESR provides a more stable marker for tracking overall inflammatory trends during treatment. This differential behavior should be considered when designing postoperative monitoring protocols for shoulder surgery and other orthopedic procedures.
Atesok et al. [4] conducted a retrospective study in 2017 to evaluate the impact of deep shoulder infections following arthroscopic RCR on patient outcomes. The study included two matched groups: 10 patients with deep shoulder infection after arthroscopic RCR and 10 control patients matched for age, sex, and tear size, who did not develop infection. The groups were compared in terms of time to initiation of physiotherapy, shoulder function, and delay in return to work. The mean time to initiation of physiotherapy was 145.3 days in the infection group compared with 40 days in the control group. The mean forward elevation of the operated shoulder was 133° in the infection group versus 172° in the control group. Furthermore, the mean time to return to preoperative work level was 5.6 months in the infection group, compared with 3 months in the control group. The authors concluded that deep shoulder infections after RCR significantly delay rehabilitation, impair shoulder function, and prolong return to work [4].
Day et al. [11] performed a retrospective study to define and compare the incidence and risk factors of short-term complications following open and arthroscopic RCR (RTCR). Using the American College of Surgeons National Surgical Quality Improvement Program database (2005–2013), they identified 11,314 RTCR procedures (24% open, 76% arthroscopic). The overall complication rate was 1.3%, with unplanned return to the operating room being the most common surgical complication (0.36%). The 30-day unplanned readmission rate was 1.16%, and mortality was 0.03%. The overall infection rate was 0.56%, with deep wound infection occurring more frequently in the open surgery group (P=0.003). Multivariate analysis identified age >65 years, operative time >90 minutes, and open RTCR as independent risk factors for complications. The authors concluded that although short-term complications after RTCR are rare, open repair is associated with a higher overall complication and infection risk [11].
Similarly, Wang et al. [12] conducted a retrospective matched-cohort study in 2022 comparing open and arthroscopic RCR with a minimum of five years of follow-up. A total of 3,266 patients undergoing open RCR were propensity-score matched with 3,266 patients undergoing arthroscopic RCR based on age, sex, Charlson comorbidity index, smoking status, and obesity. Patients who underwent open RCR had a significantly higher risk of surgical site infection within 90 days (0.89% vs 0.34%) and higher rates of manipulation under anesthesia (MUA) at both 2 years (1.65% vs 0.95%) and 5 years (1.75% vs 1.1%) compared with arthroscopic RCR. No significant differences were observed in other postoperative complications, reoperation rates, or healthcare reimbursements. The authors concluded that open RCR is associated with an increased risk of short-term infection and postoperative stiffness requiring MUA [12].
More recently, Mercurio et al. conducted a 2024 systematic review evaluating surgical management outcomes for infection following arthroscopic RCR. Five studies comprising 146 patients were included, with 71 patients (48%) managed arthroscopically and 75 patients (52%) managed with open surgery. The most common causative organism was C. acnes (50.4%) [3]. Studies reported significant postoperative improvements in ASES and Constant–Murley scores. Overall, infection eradication was achieved in 94.5% of patients, with no significant difference between arthroscopic and open revision procedures. The weighted mean duration of intravenous antibiotic therapy was 5.4±6.6 days, while the overall mean antibiotic duration (intravenous plus oral) was 40±43.5 days. The authors concluded that surgical management of infection following RCR results in high eradication rates and significant functional improvement [3].
In the present study, S. aureus was the most common causative agent of postoperative infection, although two cases of E. coli and one case of Citrobacter were also observed. The presence of gram-negative bacteria in these patients is unusual, as previous studies have typically reported S. aureus, coagulase-negative staphylococci, and P. acnes as the predominant pathogens [9, 10].
In the current study, the most commonly used antibiotic combination after debridement and drain placement was imipenem and vancomycin, prescribed to >40% of patients. Other regimens included meropenem + vancomycin, clindamycin + tigecycline, imipenem + tigecycline, and amikacin + cefepime, with an average treatment duration of two weeks. These findings reflect an aggressive approach to simultaneously cover resistant gram-positive and gram-negative organisms.
Previous studies have similarly emphasized the importance of broad-spectrum antibiotics during the early stages of treatment. Kwon et al. [2] reported that patients with early postoperative infections after RCR received antibiotics for an average of 8.7 weeks, initially targeting skin flora (Staphylococcus spp. and P. acnes). Smith et al. [8] also noted that prophylaxis and culture-guided targeted therapy are key to successful infection control. Shi et al. [9] highlighted the importance of selecting antibiotics specific to prevalent organisms and continuing treatment until inflammatory markers (ESR and CRP) normalize.
In our study, the use of imipenem and vancomycin reflects an effort to simultaneously cover resistant gram-positive bacteria (MRSA and coagulase-negative staphylococci) and gram-negative organisms (E. coli and Citrobacter), consistent with our microbiological findings. However, prolonged use of carbapenems (imipenem, meropenem) and glycopeptides (vancomycin, teicoplanin) may contribute to antibiotic resistance and adverse effects. Kadler et al. [13] reported that P. acnes is often resistant to metronidazole but sensitive to penicillins and clindamycin. Accordingly, simpler regimens may suffice when P. acnes predominates. Crane et al. [14] also demonstrated that P. acnes, a common shoulder pathogen, is highly sensitive to penicillins and first-generation cephalosporins, with variable resistance to clindamycin and vancomycin. These findings highlight the importance of tailoring antibiotic selection based on culture results and susceptibility patterns, as routine use of broad-spectrum agents may be overly conservative and increase the risk of resistance.
This study has several strengths. First, the dynamic changes in ESR and CRP were precisely recorded and analyzed throughout treatment, a feature rarely reported in similar studies. Second, detailed microbiological data revealed not only S. aureus but also unusual gram-negative organisms (E. coli, Citrobacter). Third, treatment information, including type and duration of antibiotics, was fully reported, providing an average treatment duration of two weeks that allows comparison with international protocols. Fourth, the comprehensiveness of clinical (symptoms, debridement, drain placement) and laboratory (ESR, CRP, cultures) data enhances the relevance of findings for both clinicians and researchers.
However, this study has limitations. The small sample size (14patients) reduces statistical power, rendering the results primarily descriptive. Over half of the cultures were negative, possibly due to limitations of culture techniques or undetected organisms such as P. acnes. The relatively short antibiotic duration (two weeks) may differ from international recommendations (6–8 weeks), potentially affecting outcomes. Finally, the lack of long-term follow-up on functional outcomes (pain, range of motion, return to work) limits evaluation of the clinical impact of treatment.
Conclusion
The present study demonstrated that deep infections following RCR, though rare, can lead to significant clinical consequences. ESR showed a slower but more stable decline, while CRP showed a more rapid and sensitive change, highlighting the value of using both markers for diagnosis and monitoring. Microbiological cultures identified S. aureus as the main pathogen, with occasional gram-negative bacteria (E. coli, Citrobacter), reflecting patient or hospital-specific factors. Combination antibiotic regimens, particularly imipenem and vancomycin, were effective for an average of two weeks, although longer treatment is often recommended internationally. Patient comorbidities, including diabetes, hypertension, hyperlipidemia, and ischemic heart disease, may contribute as risk factors. Despite limitations in sample size and follow-up, these findings provide valuable insights into trends in inflammatory markers, causative organisms, and treatment strategies, informing future research and optimizing postoperative infection management.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.FMD.REC.1404.074).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
Rotator cuff repair (RCR) is a commonly performed orthopaedic procedure for symptomatic rotator cuff tears, which are a frequent cause of shoulder pain and dysfunction worldwide [1]. Although operative repair generally achieves good clinical outcomes, postoperative complications can occur [2]. Deep infection is one of the most serious but relatively rare complications, with a reported incidence ranging between approximately 0.3% and 3.4% after rotator cuff surgery [3].
Deep infections after RCR may present with increasing shoulder pain, stiffness, swelling, local erythema, and systemic signs depending on severity. Because the glenohumeral joint is relatively deep and surrounded by soft tissue, clinical signs may be subtle, and definitive diagnosis often requires laboratory and microbiological evaluation. Elevated inflammatory markers, such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), are commonly used as surrogate markers of infection and treatment response. However, these markers are nonspecific and must be interpreted in conjunction with clinical findings [4-6].
The microbiological profile of postoperative shoulder infections includes various organisms. Traditional pathogens, such as Staphylococcus aureus and coagulase-negative staphylococci, have been reported. However, the anaerobic skin commensal Cutibacterium acnes (formerly Propionibacterium acnes) has emerged as a frequent isolate in deep shoulder infections following RCR, particularly in arthroscopic cases [3].
The management of deep infections after RCR typically involves a combination of surgical debridement, irrigation, drainage placement, and targeted antibiotic therapy. Prompt and aggressive treatment is crucial to eradicate the infection, prevent further soft tissue damage (including chondral destruction and muscle compromise), and improve functional outcomes. However, published literature is limited regarding comparative outcomes of open versus arthroscopic management, patterns of laboratory marker changes, and optimal antibiotic regimens in this specific clinical setting [3].
Given the potential for significant morbidity associated with infection after RCR and the relatively limited focused evidence, further investigation into clinical and laboratory outcomes following standardized treatment protocols is warranted [7]. Therefore, this study aimed to evaluate the effects of surgical debridement, prolonged drainage, and intravenous antibiotic therapy on ESR and CRP levels in patients with postoperative infection following open or arthroscopic RCR, and to characterize the microbiological profile of the infecting agents.
Methods
This retrospective cross-sectional study was conducted at Shafayahyaeian and Iranmehr Hospitals, two tertiary referral centers in Tehran Province, Iran. The study protocol was approved by the Ethics Committee of Iran University of Medical Sciences. All patients who presented between 2017 and 2024 with postoperative infection following surgical repair of a rotator cuff tear were considered for inclusion. Eligible patients were identified through review of hospital medical records. The inclusion criteria consisted of a history of rotator cuff tendon repair performed by either open surgery or arthroscopically, and a confirmed infection related to the prior RCR. Patients with incomplete or missing medical records were excluded from the study. A convenience sampling method was used, and all patients meeting the inclusion criteria during the study period were enrolled. Data were retrospectively collected through a review of medical records. The extracted variables included demographic characteristics (age and sex), comorbid conditions, such as diabetes mellitus and hypertension, type of primary RCR (open or arthroscopic), type and duration of intravenous antibiotic therapy, and microbiological findings based on culture results. Clinical evaluation of treatment success was performed by monitoring laboratory inflammatory markers, including ESR and CRP. These markers were recorded at three time points: prior to surgical intervention, one week after initiation of intravenous antibiotic therapy, and at hospital discharge. The type and duration of intravenous antibiotic therapy were also documented.
Statistical analysis
Statistical analyses were performed using the SPSS software, version 24 (IBM Corp., Armonk, NY, USA). Continuous variables were reported as Mean±SD, along with minimum and maximum values. A repeated-measures analysis was used to evaluate changes in ESR and CRP levels across the three time points (preoperative, one week after antibiotic initiation, and discharge). A P<0.05 was considered statistically significant. Patient confidentiality was strictly maintained, and all data were anonymized prior to analysis.
Surgical procedure
Following confirmation of infection, patients were transferred to the operating room for irrigation and debridement under general anesthesia in a semi-sitting position. The previous surgical incision was reopened. Granulation tissue located beneath the deltoid muscle and within the glenohumeral joint was identified and sampled for microbiological culture and pathological evaluation. All previously implanted suture materials were removed. Necrotic and infected tissues were thoroughly debrided, followed by extensive irrigation. The rotator cuff was repaired using nylon sutures. The long head of the biceps tendon was tenodesed. The coracoacromial ligament and deltoid muscle were repaired using nylon sutures. Two drains were inserted at the infection site—one intra-articular and one beneath the deltoid muscle. The skin was closed using nylon sutures, and the shoulder was immobilized with a sling. Drains were maintained for three weeks to facilitate continuous evacuation of infectious secretions. Intravenous antibiotic therapy was administered and adjusted according to culture results and continued until clinical improvement was achieved.
Results
A total of 14 patients who underwent surgical intervention for postoperative infection following open RCR between 2017 and 2024 at Shafayahyaeian and Iranmehr hospitals were included in the study. The cohort consisted of 10 men (71.4%) and 4 women (28.6%) with a mean age of 58.5±6.32 years (range, 45–66 years).
Regarding baseline comorbidities, five patients (33.3%) had diabetes mellitus, five patients (33.3%) had hypertension, four patients (26.6%) had hyperlipidemia, and three patients (20%) had ischemic heart disease. Two patients had three comorbidities, four patients had two, and five patients (33.3%) had no documented underlying diseases (Table 1).
Microbiological findings
Microbiological culture results demonstrated that S. aureus was identified in three patients (20%), Escherichia coli in two patients (13.3%), and Citrobacter species in one patient (6.6%). In eight patients (53.3%), no specific organism was isolated from culture specimens (Table 2).
Antibiotic therapy
Following surgical debridement and drain placement, the most commonly administered antibiotic regimen was a combination of imipenem and vancomycin, which was used in six patients (42.8%). Other antibiotic combinations included meropenem plus vancomycin in three patients (21.4%), clindamycin plus teicoplanin (targocid) in two patients (14.3%), imipenem plus teicoplanin in two patients (14.3%), and amikacin plus cefepime in one patient (7.2%) (Table 3).
The mean duration of intravenous antibiotic therapy was approximately two weeks in the majority of patients, with extended treatment up to three weeks in selected cases. At discharge, patients were transitioned to oral antibiotic regimens tailored according to culture results and clinical response.
One patient required modification of the antibiotic regimen due to persistent elevation of inflammatory markers, necessitating the addition of meropenem and cotrimoxazole. In another case (patient 7), no drain was placed during the initial surgery. This patient demonstrated an increase in ESR and CRP one week after antibiotic initiation and subsequently underwent a second surgical intervention with drain placement. The antibiotic regimen was modified to linezolid and rifampin, with amikacin added four days later.
Laboratory outcomes
Normality testing using the Kolmogorov–Smirnov test demonstrated that ESR and CRP values at all measured time points followed a normal distribution (all P>0.05), allowing for parametric analysis (Tables 4, 5, and 6).
A repeated-measures analysis was performed to evaluate changes in inflammatory markers over time (preoperatively, one week after initiation of antibiotic therapy, and at discharge).
The mean preoperative ESR was 61.78±23.17 mm/h. One week after the initiation of antibiotic therapy, ESR decreased to 53.86±26.33 mm/h, representing a mean reduction of 7.93 mm/hour from baseline (95% confidence interval [CI], 1.77%, 14.08%; P=0.011). At discharge, ESR further decreased to 37.43±17.29 mm/h, corresponding to a mean reduction of 24.36 mm/h relative to baseline (95% CI, 16.63%, 32.07%; P<0.001).
The mean preoperative CRP level was 54.93±39.28 mg/L. One week after antibiotic initiation, CRP decreased to 35.74±32.74 mg/L; however, this reduction did not reach statistical significance compared with baseline (mean difference: 19.93 mg/L; 95% CI, −0.003%, 39.86%; P=0.050). At discharge, CRP significantly decreased to 10.5±4.82 mg/L, reflecting a mean reduction of 44.43 mg/L compared to preoperative values (95% CI, 17.46%, 71.38%; P=0.002).
Overall, ESR levels decreased significantly both one week after antibiotic therapy and at discharge, whereas CRP levels decreased significantly only at discharge.
Discussion
The results of the present study demonstrated that the combined use of drains and antibiotics for an average of two weeks effectively reduced CRP and ESR levels. The most common microorganism responsible for secondary infection was S. aureus. In contrast, the most frequently used antibiotic regimen for infection control was a combination of imipenem and vancomycin, administered to approximately half of the patients.
Kwon et al. [2] investigated 14 patients with early-onset infections (<6 weeks) and reported that the most frequent clinical manifestations included wound discharge and local erythema, while white blood cell counts often remained within normal ranges. In that study, ESR was elevated in all patients, and CRP levels were abnormal in the evaluated cases. The authors emphasized that CRP decreases more rapidly than ESR and is therefore more useful for early diagnosis, whereas ESR decreases more slowly and is better suited for long-term monitoring [2]. Our findings align with this pattern, demonstrating a faster reduction in CRP at discharge and a more sustained decrease in ESR throughout treatment.
Similarly, a systematic review by Smith et al. [8] encompassing over 10,000 RCRs found that CRP was elevated in 83% of patients with infection, whereas ESR was elevated in only 25%. The study concluded that CRP is a more sensitive marker for detecting acute infections, while ESR may remain normal in many patients. A comparison of our data with that of this review suggests that using both markers concurrently can improve the accuracy of infection diagnosis and treatment monitoring.
Shi et al. [9] also highlighted the importance of combining traditional methods (ESR, CRP, cultures) with advanced techniques, such as PCR and sonication, for more accurate diagnosis of shoulder infections. This study demonstrated that CRP is particularly valuable for evaluating the initial response to treatment, whereas ESR is more suitable for long-term monitoring. Our findings corroborate this conclusion, indicating that a decrease in CRP at discharge can be considered a marker of successful treatment.
In contrast, Mirzayan et al. [10] evaluated patients with chronic infections (mean 9.7 months post-surgery) and reported that these patients typically presented with elevated ESR and normal white blood cell counts. Infection control often required multiple debridements, sometimes including muscle flaps. Although the infection was eventually controlled, many patients experienced significant functional limitations. These findings underscore the importance of early diagnosis and intervention, as delays may lead to soft-tissue and bone destruction and poor functional outcomes.
Overall, our findings confirm that CRP is more suitable for early diagnosis and rapid assessment of treatment response, whereas ESR provides a more stable marker for tracking overall inflammatory trends during treatment. This differential behavior should be considered when designing postoperative monitoring protocols for shoulder surgery and other orthopedic procedures.
Atesok et al. [4] conducted a retrospective study in 2017 to evaluate the impact of deep shoulder infections following arthroscopic RCR on patient outcomes. The study included two matched groups: 10 patients with deep shoulder infection after arthroscopic RCR and 10 control patients matched for age, sex, and tear size, who did not develop infection. The groups were compared in terms of time to initiation of physiotherapy, shoulder function, and delay in return to work. The mean time to initiation of physiotherapy was 145.3 days in the infection group compared with 40 days in the control group. The mean forward elevation of the operated shoulder was 133° in the infection group versus 172° in the control group. Furthermore, the mean time to return to preoperative work level was 5.6 months in the infection group, compared with 3 months in the control group. The authors concluded that deep shoulder infections after RCR significantly delay rehabilitation, impair shoulder function, and prolong return to work [4].
Day et al. [11] performed a retrospective study to define and compare the incidence and risk factors of short-term complications following open and arthroscopic RCR (RTCR). Using the American College of Surgeons National Surgical Quality Improvement Program database (2005–2013), they identified 11,314 RTCR procedures (24% open, 76% arthroscopic). The overall complication rate was 1.3%, with unplanned return to the operating room being the most common surgical complication (0.36%). The 30-day unplanned readmission rate was 1.16%, and mortality was 0.03%. The overall infection rate was 0.56%, with deep wound infection occurring more frequently in the open surgery group (P=0.003). Multivariate analysis identified age >65 years, operative time >90 minutes, and open RTCR as independent risk factors for complications. The authors concluded that although short-term complications after RTCR are rare, open repair is associated with a higher overall complication and infection risk [11].
Similarly, Wang et al. [12] conducted a retrospective matched-cohort study in 2022 comparing open and arthroscopic RCR with a minimum of five years of follow-up. A total of 3,266 patients undergoing open RCR were propensity-score matched with 3,266 patients undergoing arthroscopic RCR based on age, sex, Charlson comorbidity index, smoking status, and obesity. Patients who underwent open RCR had a significantly higher risk of surgical site infection within 90 days (0.89% vs 0.34%) and higher rates of manipulation under anesthesia (MUA) at both 2 years (1.65% vs 0.95%) and 5 years (1.75% vs 1.1%) compared with arthroscopic RCR. No significant differences were observed in other postoperative complications, reoperation rates, or healthcare reimbursements. The authors concluded that open RCR is associated with an increased risk of short-term infection and postoperative stiffness requiring MUA [12].
More recently, Mercurio et al. conducted a 2024 systematic review evaluating surgical management outcomes for infection following arthroscopic RCR. Five studies comprising 146 patients were included, with 71 patients (48%) managed arthroscopically and 75 patients (52%) managed with open surgery. The most common causative organism was C. acnes (50.4%) [3]. Studies reported significant postoperative improvements in ASES and Constant–Murley scores. Overall, infection eradication was achieved in 94.5% of patients, with no significant difference between arthroscopic and open revision procedures. The weighted mean duration of intravenous antibiotic therapy was 5.4±6.6 days, while the overall mean antibiotic duration (intravenous plus oral) was 40±43.5 days. The authors concluded that surgical management of infection following RCR results in high eradication rates and significant functional improvement [3].
In the present study, S. aureus was the most common causative agent of postoperative infection, although two cases of E. coli and one case of Citrobacter were also observed. The presence of gram-negative bacteria in these patients is unusual, as previous studies have typically reported S. aureus, coagulase-negative staphylococci, and P. acnes as the predominant pathogens [9, 10].
In the current study, the most commonly used antibiotic combination after debridement and drain placement was imipenem and vancomycin, prescribed to >40% of patients. Other regimens included meropenem + vancomycin, clindamycin + tigecycline, imipenem + tigecycline, and amikacin + cefepime, with an average treatment duration of two weeks. These findings reflect an aggressive approach to simultaneously cover resistant gram-positive and gram-negative organisms.
Previous studies have similarly emphasized the importance of broad-spectrum antibiotics during the early stages of treatment. Kwon et al. [2] reported that patients with early postoperative infections after RCR received antibiotics for an average of 8.7 weeks, initially targeting skin flora (Staphylococcus spp. and P. acnes). Smith et al. [8] also noted that prophylaxis and culture-guided targeted therapy are key to successful infection control. Shi et al. [9] highlighted the importance of selecting antibiotics specific to prevalent organisms and continuing treatment until inflammatory markers (ESR and CRP) normalize.
In our study, the use of imipenem and vancomycin reflects an effort to simultaneously cover resistant gram-positive bacteria (MRSA and coagulase-negative staphylococci) and gram-negative organisms (E. coli and Citrobacter), consistent with our microbiological findings. However, prolonged use of carbapenems (imipenem, meropenem) and glycopeptides (vancomycin, teicoplanin) may contribute to antibiotic resistance and adverse effects. Kadler et al. [13] reported that P. acnes is often resistant to metronidazole but sensitive to penicillins and clindamycin. Accordingly, simpler regimens may suffice when P. acnes predominates. Crane et al. [14] also demonstrated that P. acnes, a common shoulder pathogen, is highly sensitive to penicillins and first-generation cephalosporins, with variable resistance to clindamycin and vancomycin. These findings highlight the importance of tailoring antibiotic selection based on culture results and susceptibility patterns, as routine use of broad-spectrum agents may be overly conservative and increase the risk of resistance.
This study has several strengths. First, the dynamic changes in ESR and CRP were precisely recorded and analyzed throughout treatment, a feature rarely reported in similar studies. Second, detailed microbiological data revealed not only S. aureus but also unusual gram-negative organisms (E. coli, Citrobacter). Third, treatment information, including type and duration of antibiotics, was fully reported, providing an average treatment duration of two weeks that allows comparison with international protocols. Fourth, the comprehensiveness of clinical (symptoms, debridement, drain placement) and laboratory (ESR, CRP, cultures) data enhances the relevance of findings for both clinicians and researchers.
However, this study has limitations. The small sample size (14patients) reduces statistical power, rendering the results primarily descriptive. Over half of the cultures were negative, possibly due to limitations of culture techniques or undetected organisms such as P. acnes. The relatively short antibiotic duration (two weeks) may differ from international recommendations (6–8 weeks), potentially affecting outcomes. Finally, the lack of long-term follow-up on functional outcomes (pain, range of motion, return to work) limits evaluation of the clinical impact of treatment.
Conclusion
The present study demonstrated that deep infections following RCR, though rare, can lead to significant clinical consequences. ESR showed a slower but more stable decline, while CRP showed a more rapid and sensitive change, highlighting the value of using both markers for diagnosis and monitoring. Microbiological cultures identified S. aureus as the main pathogen, with occasional gram-negative bacteria (E. coli, Citrobacter), reflecting patient or hospital-specific factors. Combination antibiotic regimens, particularly imipenem and vancomycin, were effective for an average of two weeks, although longer treatment is often recommended internationally. Patient comorbidities, including diabetes, hypertension, hyperlipidemia, and ischemic heart disease, may contribute as risk factors. Despite limitations in sample size and follow-up, these findings provide valuable insights into trends in inflammatory markers, causative organisms, and treatment strategies, informing future research and optimizing postoperative infection management.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.FMD.REC.1404.074).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
References
- Yeranosian MG, Arshi A, Terrell RD, Wang JC, McAllister DR, Petrigliano FA. Incidence of acute postoperative infections requiring reoperation after arthroscopic shoulder surgery. Am J Sports Med. 2014; 42(2):437-41. [DOI:10.1177/0363546513510686] [PMID]
- Kwon YW, Kalainov DM, Rose HA, Bisson LJ, Weiland AJ. Management of early deep infection after rotator cuff repair surgery. J Shoulder Elbow Surg. 2005; 14(1):1-5. [DOI:10.1016/j.jse.2004.04.010] [PMID]
- Mercurio M, Gasparini G, Cofano E, Colace S, Galasso O. Revision surgery for shoulder infection after arthroscopic rotator cuff repair: Functional outcomes and eradication rate-a systematic review. Healthcare. 2024. [DOI:10.3390/healthcare12131291] [PMID]
- Atesok K, MacDonald P, Leiter J, McRae S, Stranges G, Old J. Postoperative deep shoulder infections following rotator cuff repair. World J Orthop. 2017; 8(8):612. [DOI:10.5312/wjo.v8.i8.612] [PMID]
- Dodson CC, Craig EV, Cordasco FA, Dines DM, Dines JS, DiCarlo E, et al. Propionibacterium acnes infection after shoulder arthroplasty: A diagnostic challenge. J Shoulder Elbow Surg. 2010; 19(2):303-7. [DOI:10.1016/j.jse.2009.07.065] [PMID]
- Padegimas EM, Lawrence C, Narzikul AC, Zmistowski BM, Abboud JA, Williams GR, et al. Future surgery after revision shoulder arthroplasty: The impact of unexpected positive cultures. J Shoulder Elbow Surg. 2017; 26(6):975-81. [DOI:10.1016/j.jse.2016.10.023] [PMID]
- Athwal GS, Sperling JW, Rispoli DM, Cofield RH. Deep infection after rotator cuff repair. J Shoulder Elbow Surg. 2007; 16(3):306-11. [DOI:10.1016/j.jse.2006.05.013] [PMID]
- Smith CD, Corner T, Modi CS, Drew S. The evidence for the management of deep infection after rotator cuff repair. Shoulder Elbow. 2011; 3(3):138-42. [DOI:10.1111/j.1758-5740.2011.00114.x]
- Shi LL, von Keudell AG, Higgins LD. Treatment of shoulder infections after arthroscopy, open surgery, or arthroplasty. Curr Orthop Pract. 2012; 23(1):23-8. [DOI:10.1097/BCO.0b013e31823fe051]
- Mirzayan R, Itamura JM, Vangsness Jr T, Holtom PD, Sherman R, Patzakis MJ. Management of chronic deep infection following rotator cuff repair. JBJS. 2000; 82(8):1115. [DOI:10.2106/00004623-200008000-00008] [PMID]
- Day M, Westermann R, Duchman K, Gao Y, Pugely A, Bollier M, et al. Comparison of Short-term Complications After Rotator Cuff Repair: Open Versus Arthroscopic. Arthroscopy. 2018; 34(4):1130-6. [DOI:10.1016/j.arthro.2017.10.027] [PMID]
- Wang KY, Agarwal AR, Xu AL, Best MJ, Kreulen RT, Jami M, et al. Increased risk of surgical-site infection and need for manipulation under anesthesia for those who undergo open versus arthroscopic rotator cuff repair. Arthroscopy Sports Med Rehabil. 2022; 4(2):e527-e33. [DOI:10.1016/j.asmr.2021.11.012] [PMID]
- Kadler BK, Mehta SS, Funk L. Propionibacterium acnes infection after shoulder surgery. Int J Shoulder Surg. 2015; 9(4):139. [DOI:10.4103/0973-6042.167957] [PMID]
- Crane JK, Hohman DW, Nodzo SR, Duquin TR. Antimicrobial susceptibility of Propionibacterium acnes isolates from shoulder surgery. Antimicrob Agents Chemother. 2013; 57(7):3424-6. [DOI:10.1128/AAC.00463-13] [PMID]
Type of Study: Research Article |
Subject:
Shoulder / Elbow
Received: 2025/03/2 | Accepted: 2025/09/27 | Published: 2025/11/1
Received: 2025/03/2 | Accepted: 2025/09/27 | Published: 2025/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
