

Volume 12, Issue 4 (Autumn 2025)
JROS 2025, 12(4): 161-170 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Torkaman A, Fathi M, Zareie B, Safaee O. Comparison of Clinical Outcomes of Intra-articular Injection of Platelet-rich Plasma Versus Hyaluronic Acid in Patients With Knee Osteoarthritis: A Systematic Review. JROS 2025; 12 (4) :161-170
URL: http://jros.iums.ac.ir/article-1-2311-en.html
URL: http://jros.iums.ac.ir/article-1-2311-en.html



1- Department of Orthopedics, Bone and Joint Reconstruction Research Center, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Knee osteoarthritis (OA), Platelet-rich plasma (PRP), Hyaluronic acid (HA), Intra-articular injection, Joint function
Full-Text [PDF 792 kb]
(81 Downloads)
| Abstract (HTML) (367 Views)
General characteristics of the included studies
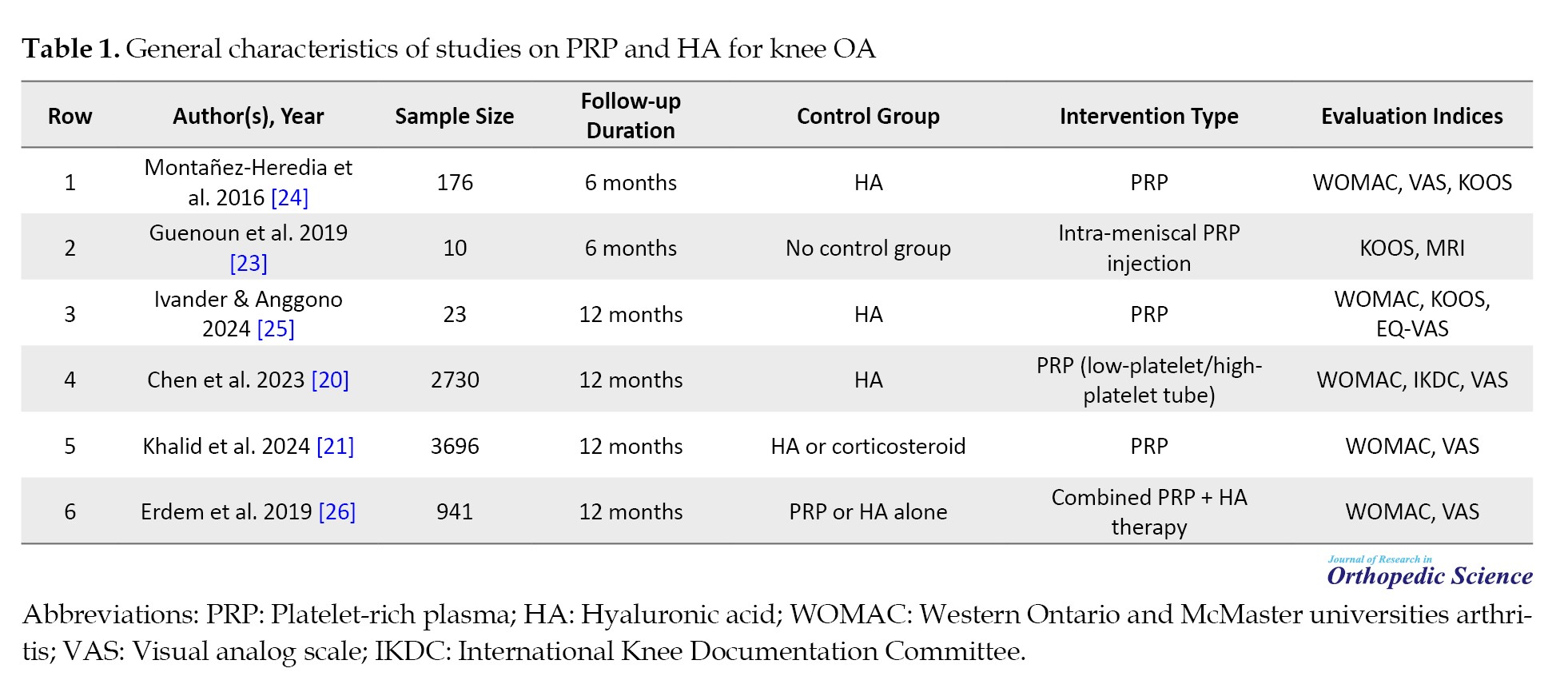
This review, encompassing studies published between 2016 and 2024, evaluated the evidence on the efficacy of PRP injections for patients with mild-to-moderate knee OA or degenerative meniscal tears, with a mean age of 40-65 years (Table 1).
Overall efficacy and relative superiority of PRP
A consensus among the reviewed studies indicates that both PRP and HA injections are effective in significantly reducing pain (measured by indices, such as VAS and the pain subscale of WOMAC) and improving knee function (measured by indices, such as WOMAC, KOOS, and IKDC). However, robust evidence from large-scale meta-analyses [20, 21] demonstrates that PRP is not only a valid therapeutic option but also generally superior in clinical outcomes. This advantage has been reported as a more rapid onset of action in symptom reduction and a longer duration of effect (lasting at least up to 12 months of follow-up) compared to HA [20, 21].
Synergistic effect of combination therapy
A significant finding highlighted in a 2019 systematic review is the potential synergistic effect of combination therapy using both PRP and HA. This finding suggests that the combination of these two agents may be more effective than using either agent alone. This phenomenon is likely attributable to complementary mechanisms of action: HA provides immediate lubrication and visco-supplementation, while PRP actively stimulates tissue repair and regeneration processes through the release of numerous growth factors [22].
The challenge of heterogeneity and standardization
A major obstacle to drawing definitive conclusions and making direct comparisons across studies is the substantial heterogeneity in PRP preparation and injection protocols. Variables such as the type of kit used (yielding leukocyte-poor PRP (LP-PRP), versus LR-PRP, the number and intervals of injections, and the injected volume varied considerably among the studies. This heterogeneity is recognized as a key factor contributing to the differences in reported outcomes and underscores the pressing need for standardized treatment protocols in future research.
Although most studies have focused on knee OA, Guenoun et al. (2019) indicated that PRP applications are expanding to include intra-meniscal injuries. This suggests that PRP is also being investigated as a potential regenerative treatment for soft tissue injuries [23].
Therefore, current evidence strongly supports the efficacy of PRP in reducing pain and improving function in patients with knee OA, suggesting that this treatment may have clinical superiority over HA. However, to definitively confirm the superiority of combination therapy and to determine the optimal PRP preparation and injection protocol, it is essential to conduct well-designed clinical trials with standardized protocols.
Clinical outcomes
Comparison of the efficacy of PRP and HA:
Evidence from multiple studies indicates that both injectable treatments, PRP and HA, are effective in reducing pain and improving function in patients with degenerative meniscal tears. However, the pattern and duration of efficacy differ between the two treatments. The study by Montañez-Heredia et al. (2016) showed that although both groups achieved significant improvement by the end of the 6-month follow-up period, the PRP group experienced a faster rate of improvement during the first three months. This finding suggests that PRP may be particularly useful for achieving a rapid clinical response in the early stages of the disease [24].
Guenoun et al. (2019), investigating intra-meniscal PRP injection, confirmed its efficacy in a more specialized context. This study reported an increase in the KOOS from 56.6 to 72.7 and observed a quicker return to sports activities. These results position PRP as a promising, minimally invasive intervention for meniscal tissue repair [23].
Long-term superiority of PRP and large-scale studies:
Large meta-analyses with high sample sizes provided stronger evidence of PRP superiority. Chen et al. (2023), which analyzed data from 2,730 patients, consistently showed that PRP led to better WOMAC and IKDC scores compared to HA. An important finding of this study was the impact of PRP preparation type, where LP-PRP demonstrated superior clinical performance compared to LR-PRP. This highlights the importance of standardizing PRP formulations [20].
Similarly, a meta-analysis by Khalid et al. (2024), including 3,696 patients, concluded that PRP is not only more effective than HA in reducing pain and improving function, but these effects remain stable for up to 12 months. This study introduces PRP as a first-line non-surgical option for managing these patients [21].
Potential for synergistic effect of combination therapy:
An interesting area of research is the investigation of combination therapy. A previous systematic review reported that this regimen led to greater improvement in WOMAC and VAS scores than either agent alone. This synergistic effect is likely due to complementary mechanisms of action: HA provides immediate lubrication and cartilage protection, while PRP creates a restorative and anti-inflammatory environment by releasing growth factors [26].
Safety and adverse effects:
The safety profile of both PRP and HA treatments has been evaluated as favorable. As summarized in Table 2, the adverse effects reported across all studies were limited, mild, and transient.
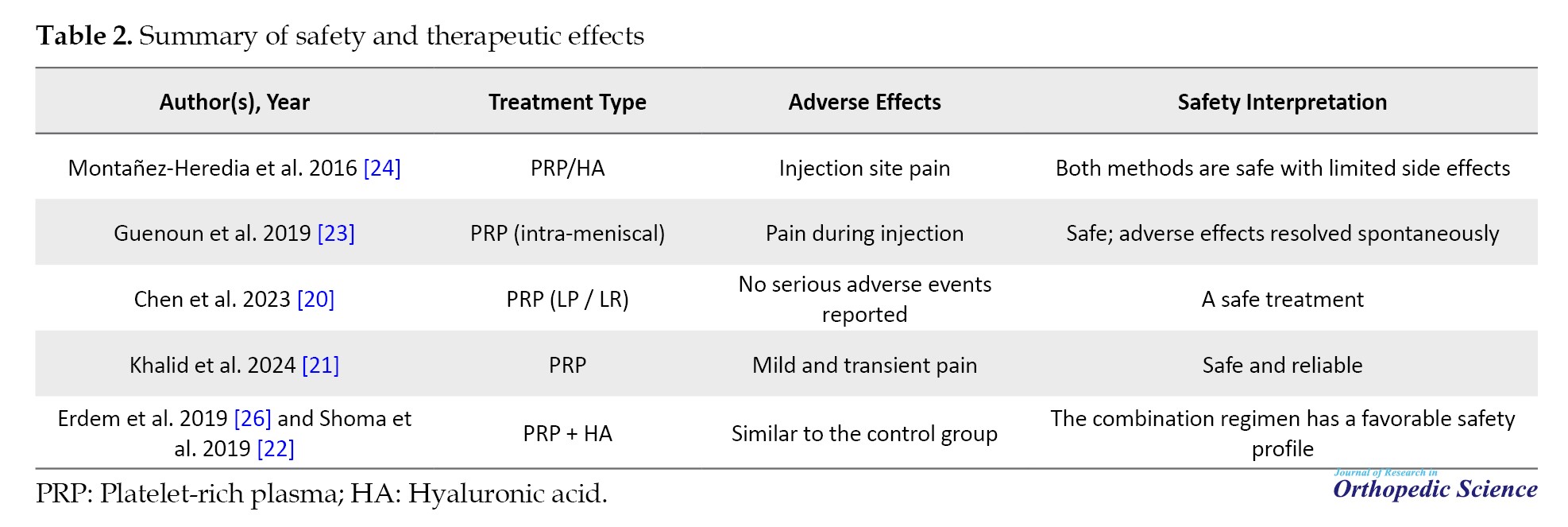
The most common adverse effect was temporary pain or swelling at the injection site, which typically resolved spontaneously within 24-72 hours. Large studies, including Chen et al. (2023) [18] and Khalid et al. (2024) [19], reported no serious or systemic treatment-related adverse events. Furthermore, a study on PRP+HA combination therapy showed that adding PRP to HA did not alter the safety profile, and its adverse effects were similar to those of the control group [26]. These findings generally indicate that intra-articular injections of PRP and HA are safe and acceptable interventions with low adverse event rates.
Discussion
This systematic review aimed to evaluate the efficacy and safety of PRP and HA, used as monotherapies or in combination, for the treatment of knee OA. The results indicated that both treatment methods led to significant improvements in patients’ clinical indices, including WOMAC, VAS, IKDC, EQ-VAS, and Tegner scores [27-29]. Overall, no significant difference was observed between PRP and HA in terms of pain relief or safety during long-term follow-up, consistent with previous studies [29].
However, subgroup and longitudinal analyses revealed that PRP, particularly LP-PRP formulations, improved total IKDC and WOMAC scores compared to HA and LR-PRP, suggesting that PRP may offer greater long-term functional benefits [30, 31]. These findings are also consistent with biological mechanisms, as PRP contains growth factors that stimulate chondrocyte proliferation, regulate collagenase activity, and promote synthesis of the extracellular matrix. In contrast, HA lacks such regenerative effects [27]. Furthermore, the lower retreatment rate in the PRP group at 24 months may be clinically relevant, even though no significant difference in overall effect duration was observed [32].
The efficacy of PRP is influenced by variables such as leukocyte concentration, preparation method, and number of injections. Laboratory studies have shown that leukocytes may activate catabolic and inflammatory pathways, which can reduce long-term effects, whereas LP-PRP mitigates these negative impacts while preserving growth factor activity [33]. Additionally, using a double-spin centrifugation method for PRP preparation increases platelet and growth factor concentration, thereby enhancing therapeutic efficacy [32]. However, differences in formulations and injection protocols led to variable clinical outcomes, underscoring the necessity for standardization in this field [27].
The combination of PRP and HA may have a synergistic effect; HA contributes through lubrication and mechanical protection, while PRP provides regenerative effects, together aiding in pain reduction and functional improvement. Meta-analyses and previous studies indicate that the PRP + HA combination leads to greater reductions in WOMAC scores and better functional outcomes compared to either treatment alone, especially at long-term follow-up [34, 35]. The mechanism of this synergy may involve regulation of inflammatory cytokines, such as interleukin-1 beta (IL-1β) and tumor necrosis factor (TNF)-α, activation of TGF-β signaling pathways, and enhanced cartilage repair via CD44 and TGF-beta type II receptor (βRII) [36].
Despite these positive results, the study has limitations. Variations in follow-up duration, PRP preparation methods, injection volume, and patient characteristics (age, KL grade, degree of cartilage degeneration) can lead to heterogeneity in the results [37]. Furthermore, the limited number of long-term RCTs and incomplete reporting of adverse events prevent definitive conclusions regarding the absolute superiority of one treatment over the other. Although PRP demonstrated better long-term functional outcomes, no significant differences were observed in pain relief or safety, necessitating further studies with standardized protocols, adequate sample sizes, and follow-up periods exceeding 24 months [38].
In summary, this study confirms the efficacy of both PRP and HA in reducing Knee OA symptoms and improving knee function. LP-PRP, either alone or combined with HA, may provide greater long-term functional benefits and a lower retreatment rate compared to HA or LR-PRP, although further research is essential to optimize PRP formulations and injection strategies. The findings of this study offer important clinical insights for selecting injectable therapies for patients with knee OA and emphasize that treatment decisions should be based on biological mechanisms and individual patient characteristics [37-39].
Conclusion
The present study demonstrated that both LR-PRP and HA improve pain, joint function, and the duration of effect in patients with knee OA. However, PRP, particularly its LP-PRP, showed a tendency toward reduced reinjection requirements and greater long-term functional improvement. Both treatments were safe and well-tolerated; however, PRP’s potential for achieving more sustained clinical effects suggests it may be a preferable option for long-term symptom management. Confirming these findings and optimizing treatment strategies requires large-scale, long-term clinical trials with standardized PRP protocols.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Omid Safaee; Methodology: Bushra Zareie; Validation, formal analysis, resources, and data curation: Ali Torkaman, Mohsen Fathi Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Full-Text: (40 Views)
Introduction
Osteoarthritis (OA) is among the most prevalent joint disorders and is characterized as a chronic, progressive, and multifactorial condition [1]. It is defined by the gradual degradation of articular cartilage, osteophyte formation, alterations in the subchondral bone, and chronic synovial inflammation, ultimately leading to ‘joint failure’ [2]. Historically perceived merely as a degenerative process resulting from mechanical wear and tear, OA is now recognized as a complex phenomenon driven by the interplay of biomechanical, inflammatory, and metabolic factors that disrupt the joint tissue’s repair capacity [3].
Global reports indicate that OA affects approximately 3.3%-3.6% of the world’s population, causing moderate-to-severe disability in over 43 million individuals; consequently, it is identified as the eleventh leading cause of disability worldwide [4]. In 2024, the Osteoarthritis Research Society International published an official report designating OA as a serious disease imposing a significant burden on healthcare systems [5]. Among various joints, the knee is most frequently affected. Knee OA is particularly common in the elderly and has become a primary cause of chronic pain, functional impairment, and mobility disability [6]. Studies indicate that, after age 60, the prevalence of knee OA is higher in women (13%) than in men (10%) [7].
The primary pharmacological management for these patients typically relies on non-steroidal anti-inflammatory drugs (NSAIDs). However, long-term use of NSAIDs is associated with serious adverse effects, including gastrointestinal bleeding, hepatic injury, and other systemic complications [8]. Therefore, intra-articular injection therapies have gained attention as alternatives with a more favorable safety profile. Among these, two widely used approaches are hyaluronic acid (HA) (Hyalgan) and platelet-rich plasma (PRP) injections. HA, a natural component of synovial fluid, functions as a lubricant and shock absorber within the joint [9]. In contrast, PRP is derived from the centrifugation of autologous blood and contains a high concentration of platelets, growth factors, such as platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), epithelial growth factor (EGF), basic fibroblast growth factor (bFGF), and transforming growth factor (TGF)-β1, which stimulate tissue repair, and cartilage regeneration [10, 11].
Recent studies have indicated that PRP injections, by stimulating growth factors and modulating inflammation, can effectively reduce pain and improve knee joint function [12]. In contrast, HA exerts both mechanical and biochemical effects, enhancing joint lubrication and reducing cartilage wear [13]. However, studies have reported inconsistent findings regarding their comparative efficacy. Some studies have reported superior efficacy of PRP in improving outcomes, such as Western Ontario and McMaster universities arthritis (WOMAC), visual analog scale (VAS), and International Knee Documentation Committee (IKDC) scores [14, 15], while others have found no significant difference between PRP and HA or have even reported greater effects with HA [16]. Furthermore, the concurrent combination of PRP and HA has shown promising results in some trials, demonstrating benefits in pain reduction and enhanced cartilage regeneration [17].
Given increasing life expectancy and the rising prevalence of knee OA, the need for non-invasive, low-risk, and cost-effective treatments is more pressing than ever. In this context, comparing the clinical outcomes of intra-articular PRP and HA injections in patients with knee OA represents a significant step towards selecting the optimal therapeutic approach. The aim is to improve joint function, alleviate pain, and enhance patients’ quality of life. This systematic review analyzed and compared the efficacy of these two treatment modalities across various functional and clinical indices, including WOMAC, VAS, IKDC, Tegner, and EuroQol (EQ)-VAS scores. By synthesizing scientific evidence, this study aimed to propose an effective strategy to optimize treatment for patients with knee OA.
Methods
This systematic review was designed in accordance with preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines [18] to compare the effectiveness of intra-articular injection of PRP and HA in patients with knee OA, and its process was registered in the international prospective register of systematic reviews (PROSPERO).
Literature search
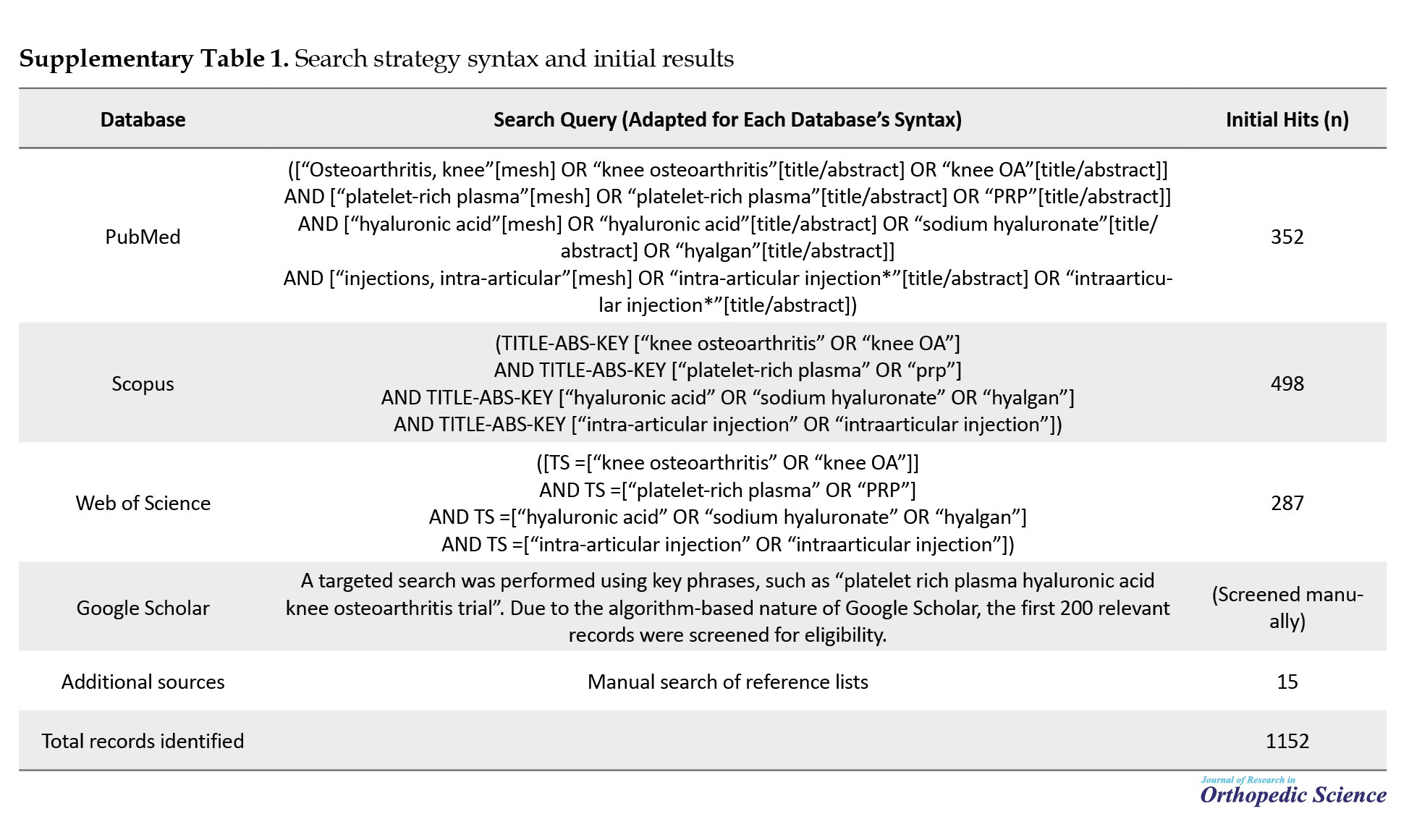
After determining the search strategy based on the patient, problem, population, intervention or exposure, comparison, control or comparator, outcome (PICO) framework, we searched PubMed/Medline, Scopus, Web of Science, and Embase databases using relevant search terms to find relevant articles. Two independent investigators searched. The search was limited to studies published between January 2010 and January 2026 to ensure the inclusion of contemporary evidence. We also searched Google Scholar and the references of the included articles as grey literature. The databases were searched using a combination of the following terms: OA, knee OA, PRP, HA, sodium hyaluronate, injections, intra-articular, intra-articular injection. The search strategy for the sources is reported separately in Supplementary Table 1.
The PICO framework was specified as follows: population: adults with knee OA, exposure: intra-articular injection of PRP, comparison: intra-articular injection of HA, and outcome: clinical and functional outcomes.
Functional or clinical outcomes were assessed using mean pre- and postoperative changes in functional score WOMAC, VAS, IKDC, and knee injury and OA outcome score (KOOS) indices.
Inclusion and exclusion criteria
Studies were selected based on the following criteria: studies that directly compared intra-articular injections of PRP and HA in patients with knee OA, clinical or quasi-experimental studies reporting clinical outcomes, such as WOMAC, VAS, or IKDC scores, studies providing clear information on sample size, injection protocol, follow-up duration, and treatment outcomes, and articles published in English or Persian. The exclusion criteria included editorials, case reports, studies without full-text access, and studies published in non-English/Persian-language journals.
Screening and study selection
The screening and selection of studies were carried out in the following steps.
1. Initial search of databases and aggregation of articles found from the databases using the statistical software EndNote
2. Identification and elimination of duplicate studies between sources using the software EndNote
3. Two independent researchers assessed the remaining articles for relevance to the research question, including the title and, if applicable, the abstract.
4. A third researcher resolved any disagreements in selecting or excluding an article. After applying the inclusion and exclusion criteria, the full texts of the remaining articles were reviewed.
Data extraction
Initially, variables for extraction were identified by a committee of orthopedic surgeons and epidemiologists, as well as by a literature review. Data extraction was performed independently by two investigators using Microsoft Excel. A third investigator resolved any disagreements between the two investigators.
The extracted variables included the following: authors, year of publication, country of origin, study design, sample size, demographic characteristics of the study population (age, sex, body mass index, Kellogg-Lawrence score), type and method of PRP preparation (e.g. leukocyte-rich PRP [LR-PRP]), type and frequency of HA injections, injection protocol, duration of follow-up, and primary functional or clinical outcomes (e.g. WOMAC, VAS, IKDC, KOOS scores). Data were organized in summary tables to facilitate systematic comparison between studies.
Quality assessment
The risk of bias for each included randomized controlled trial (RCT) was assessed using the Cochrane risk of bias 2 (RoB 2) [19], which covers five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Each study was rated for risk of bias as low risk, with some concerns, or high risk, based on RoB 2 guidances.
Data analysis and synthesis
The data were analyzed qualitatively. The findings from the included studies were descriptively and comparatively analyzed by intervention type, outcome measures (e.g. WOMAC, VAS, IKDC, and Tegner scores), and follow-up duration. Commonalities, differences, and overall trends in the results were synthesized and presented in tables and analytical interpretations to provide a comprehensive overview of the relative effects of PRP and HA on the alleviation of knee OA symptoms.
Results
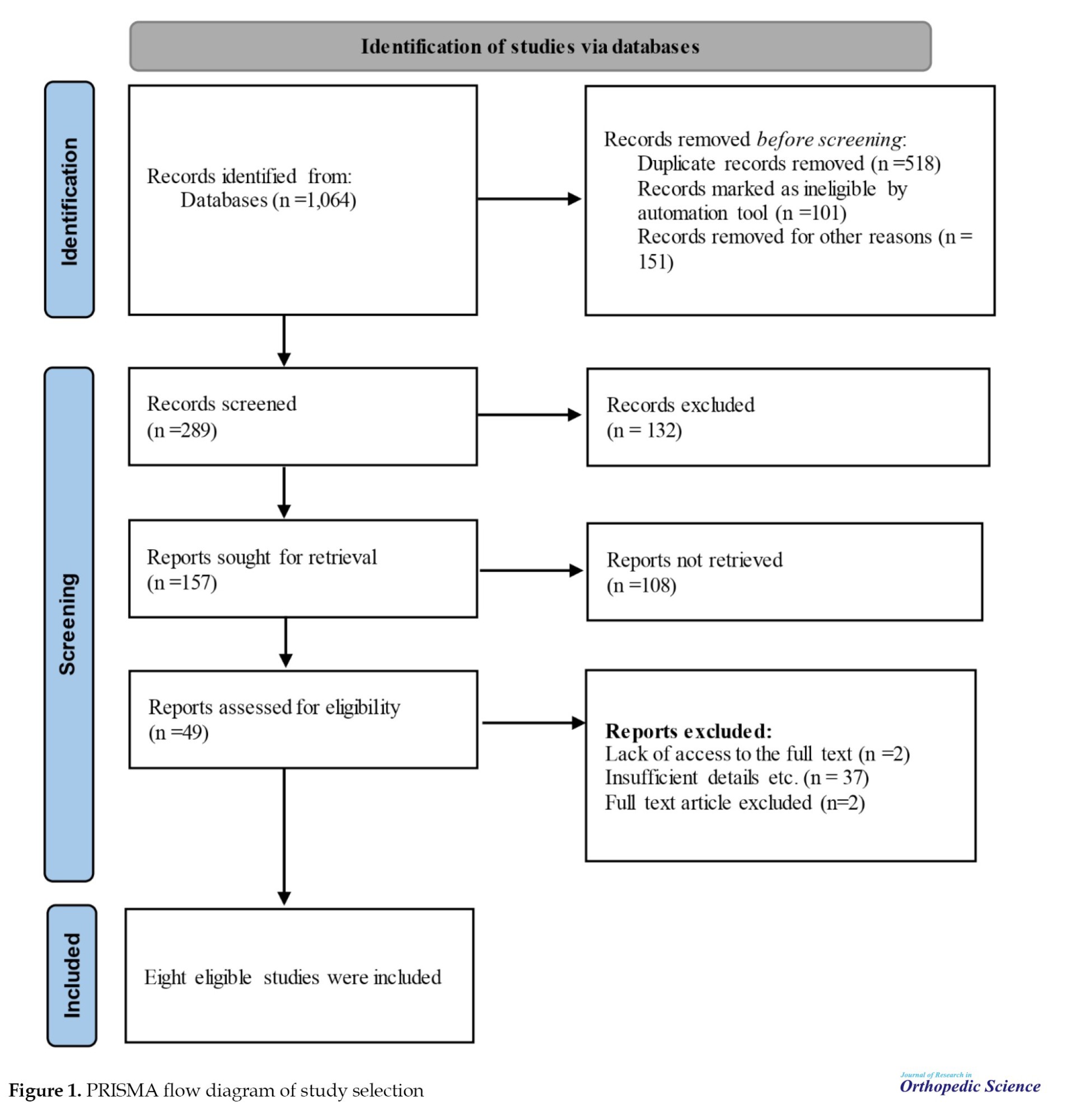
The initial search returned 1,064 results from the searched databases. After removing duplicate records, 49 articles were selected for full-text review based on their titles and abstracts. Finally, after applying the inclusion criteria, eight RCT studies were included in this systematic review for qualitative analysis (Figure 1).
Osteoarthritis (OA) is among the most prevalent joint disorders and is characterized as a chronic, progressive, and multifactorial condition [1]. It is defined by the gradual degradation of articular cartilage, osteophyte formation, alterations in the subchondral bone, and chronic synovial inflammation, ultimately leading to ‘joint failure’ [2]. Historically perceived merely as a degenerative process resulting from mechanical wear and tear, OA is now recognized as a complex phenomenon driven by the interplay of biomechanical, inflammatory, and metabolic factors that disrupt the joint tissue’s repair capacity [3].
Global reports indicate that OA affects approximately 3.3%-3.6% of the world’s population, causing moderate-to-severe disability in over 43 million individuals; consequently, it is identified as the eleventh leading cause of disability worldwide [4]. In 2024, the Osteoarthritis Research Society International published an official report designating OA as a serious disease imposing a significant burden on healthcare systems [5]. Among various joints, the knee is most frequently affected. Knee OA is particularly common in the elderly and has become a primary cause of chronic pain, functional impairment, and mobility disability [6]. Studies indicate that, after age 60, the prevalence of knee OA is higher in women (13%) than in men (10%) [7].
The primary pharmacological management for these patients typically relies on non-steroidal anti-inflammatory drugs (NSAIDs). However, long-term use of NSAIDs is associated with serious adverse effects, including gastrointestinal bleeding, hepatic injury, and other systemic complications [8]. Therefore, intra-articular injection therapies have gained attention as alternatives with a more favorable safety profile. Among these, two widely used approaches are hyaluronic acid (HA) (Hyalgan) and platelet-rich plasma (PRP) injections. HA, a natural component of synovial fluid, functions as a lubricant and shock absorber within the joint [9]. In contrast, PRP is derived from the centrifugation of autologous blood and contains a high concentration of platelets, growth factors, such as platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), epithelial growth factor (EGF), basic fibroblast growth factor (bFGF), and transforming growth factor (TGF)-β1, which stimulate tissue repair, and cartilage regeneration [10, 11].
Recent studies have indicated that PRP injections, by stimulating growth factors and modulating inflammation, can effectively reduce pain and improve knee joint function [12]. In contrast, HA exerts both mechanical and biochemical effects, enhancing joint lubrication and reducing cartilage wear [13]. However, studies have reported inconsistent findings regarding their comparative efficacy. Some studies have reported superior efficacy of PRP in improving outcomes, such as Western Ontario and McMaster universities arthritis (WOMAC), visual analog scale (VAS), and International Knee Documentation Committee (IKDC) scores [14, 15], while others have found no significant difference between PRP and HA or have even reported greater effects with HA [16]. Furthermore, the concurrent combination of PRP and HA has shown promising results in some trials, demonstrating benefits in pain reduction and enhanced cartilage regeneration [17].
Given increasing life expectancy and the rising prevalence of knee OA, the need for non-invasive, low-risk, and cost-effective treatments is more pressing than ever. In this context, comparing the clinical outcomes of intra-articular PRP and HA injections in patients with knee OA represents a significant step towards selecting the optimal therapeutic approach. The aim is to improve joint function, alleviate pain, and enhance patients’ quality of life. This systematic review analyzed and compared the efficacy of these two treatment modalities across various functional and clinical indices, including WOMAC, VAS, IKDC, Tegner, and EuroQol (EQ)-VAS scores. By synthesizing scientific evidence, this study aimed to propose an effective strategy to optimize treatment for patients with knee OA.
Methods
This systematic review was designed in accordance with preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines [18] to compare the effectiveness of intra-articular injection of PRP and HA in patients with knee OA, and its process was registered in the international prospective register of systematic reviews (PROSPERO).
Literature search
After determining the search strategy based on the patient, problem, population, intervention or exposure, comparison, control or comparator, outcome (PICO) framework, we searched PubMed/Medline, Scopus, Web of Science, and Embase databases using relevant search terms to find relevant articles. Two independent investigators searched. The search was limited to studies published between January 2010 and January 2026 to ensure the inclusion of contemporary evidence. We also searched Google Scholar and the references of the included articles as grey literature. The databases were searched using a combination of the following terms: OA, knee OA, PRP, HA, sodium hyaluronate, injections, intra-articular, intra-articular injection. The search strategy for the sources is reported separately in Supplementary Table 1.
The PICO framework was specified as follows: population: adults with knee OA, exposure: intra-articular injection of PRP, comparison: intra-articular injection of HA, and outcome: clinical and functional outcomes.
Functional or clinical outcomes were assessed using mean pre- and postoperative changes in functional score WOMAC, VAS, IKDC, and knee injury and OA outcome score (KOOS) indices.
Inclusion and exclusion criteria
Studies were selected based on the following criteria: studies that directly compared intra-articular injections of PRP and HA in patients with knee OA, clinical or quasi-experimental studies reporting clinical outcomes, such as WOMAC, VAS, or IKDC scores, studies providing clear information on sample size, injection protocol, follow-up duration, and treatment outcomes, and articles published in English or Persian. The exclusion criteria included editorials, case reports, studies without full-text access, and studies published in non-English/Persian-language journals.
Screening and study selection
The screening and selection of studies were carried out in the following steps.
1. Initial search of databases and aggregation of articles found from the databases using the statistical software EndNote
2. Identification and elimination of duplicate studies between sources using the software EndNote
3. Two independent researchers assessed the remaining articles for relevance to the research question, including the title and, if applicable, the abstract.
4. A third researcher resolved any disagreements in selecting or excluding an article. After applying the inclusion and exclusion criteria, the full texts of the remaining articles were reviewed.
Data extraction
Initially, variables for extraction were identified by a committee of orthopedic surgeons and epidemiologists, as well as by a literature review. Data extraction was performed independently by two investigators using Microsoft Excel. A third investigator resolved any disagreements between the two investigators.
The extracted variables included the following: authors, year of publication, country of origin, study design, sample size, demographic characteristics of the study population (age, sex, body mass index, Kellogg-Lawrence score), type and method of PRP preparation (e.g. leukocyte-rich PRP [LR-PRP]), type and frequency of HA injections, injection protocol, duration of follow-up, and primary functional or clinical outcomes (e.g. WOMAC, VAS, IKDC, KOOS scores). Data were organized in summary tables to facilitate systematic comparison between studies.
Quality assessment
The risk of bias for each included randomized controlled trial (RCT) was assessed using the Cochrane risk of bias 2 (RoB 2) [19], which covers five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Each study was rated for risk of bias as low risk, with some concerns, or high risk, based on RoB 2 guidances.
Data analysis and synthesis
The data were analyzed qualitatively. The findings from the included studies were descriptively and comparatively analyzed by intervention type, outcome measures (e.g. WOMAC, VAS, IKDC, and Tegner scores), and follow-up duration. Commonalities, differences, and overall trends in the results were synthesized and presented in tables and analytical interpretations to provide a comprehensive overview of the relative effects of PRP and HA on the alleviation of knee OA symptoms.
Results
The initial search returned 1,064 results from the searched databases. After removing duplicate records, 49 articles were selected for full-text review based on their titles and abstracts. Finally, after applying the inclusion criteria, eight RCT studies were included in this systematic review for qualitative analysis (Figure 1).
General characteristics of the included studies
This review, encompassing studies published between 2016 and 2024, evaluated the evidence on the efficacy of PRP injections for patients with mild-to-moderate knee OA or degenerative meniscal tears, with a mean age of 40-65 years (Table 1).
Overall efficacy and relative superiority of PRP
A consensus among the reviewed studies indicates that both PRP and HA injections are effective in significantly reducing pain (measured by indices, such as VAS and the pain subscale of WOMAC) and improving knee function (measured by indices, such as WOMAC, KOOS, and IKDC). However, robust evidence from large-scale meta-analyses [20, 21] demonstrates that PRP is not only a valid therapeutic option but also generally superior in clinical outcomes. This advantage has been reported as a more rapid onset of action in symptom reduction and a longer duration of effect (lasting at least up to 12 months of follow-up) compared to HA [20, 21].
Synergistic effect of combination therapy
A significant finding highlighted in a 2019 systematic review is the potential synergistic effect of combination therapy using both PRP and HA. This finding suggests that the combination of these two agents may be more effective than using either agent alone. This phenomenon is likely attributable to complementary mechanisms of action: HA provides immediate lubrication and visco-supplementation, while PRP actively stimulates tissue repair and regeneration processes through the release of numerous growth factors [22].
The challenge of heterogeneity and standardization
A major obstacle to drawing definitive conclusions and making direct comparisons across studies is the substantial heterogeneity in PRP preparation and injection protocols. Variables such as the type of kit used (yielding leukocyte-poor PRP (LP-PRP), versus LR-PRP, the number and intervals of injections, and the injected volume varied considerably among the studies. This heterogeneity is recognized as a key factor contributing to the differences in reported outcomes and underscores the pressing need for standardized treatment protocols in future research.
Although most studies have focused on knee OA, Guenoun et al. (2019) indicated that PRP applications are expanding to include intra-meniscal injuries. This suggests that PRP is also being investigated as a potential regenerative treatment for soft tissue injuries [23].
Therefore, current evidence strongly supports the efficacy of PRP in reducing pain and improving function in patients with knee OA, suggesting that this treatment may have clinical superiority over HA. However, to definitively confirm the superiority of combination therapy and to determine the optimal PRP preparation and injection protocol, it is essential to conduct well-designed clinical trials with standardized protocols.
Clinical outcomes
Comparison of the efficacy of PRP and HA:
Evidence from multiple studies indicates that both injectable treatments, PRP and HA, are effective in reducing pain and improving function in patients with degenerative meniscal tears. However, the pattern and duration of efficacy differ between the two treatments. The study by Montañez-Heredia et al. (2016) showed that although both groups achieved significant improvement by the end of the 6-month follow-up period, the PRP group experienced a faster rate of improvement during the first three months. This finding suggests that PRP may be particularly useful for achieving a rapid clinical response in the early stages of the disease [24].
Guenoun et al. (2019), investigating intra-meniscal PRP injection, confirmed its efficacy in a more specialized context. This study reported an increase in the KOOS from 56.6 to 72.7 and observed a quicker return to sports activities. These results position PRP as a promising, minimally invasive intervention for meniscal tissue repair [23].
Long-term superiority of PRP and large-scale studies:
Large meta-analyses with high sample sizes provided stronger evidence of PRP superiority. Chen et al. (2023), which analyzed data from 2,730 patients, consistently showed that PRP led to better WOMAC and IKDC scores compared to HA. An important finding of this study was the impact of PRP preparation type, where LP-PRP demonstrated superior clinical performance compared to LR-PRP. This highlights the importance of standardizing PRP formulations [20].
Similarly, a meta-analysis by Khalid et al. (2024), including 3,696 patients, concluded that PRP is not only more effective than HA in reducing pain and improving function, but these effects remain stable for up to 12 months. This study introduces PRP as a first-line non-surgical option for managing these patients [21].
Potential for synergistic effect of combination therapy:
An interesting area of research is the investigation of combination therapy. A previous systematic review reported that this regimen led to greater improvement in WOMAC and VAS scores than either agent alone. This synergistic effect is likely due to complementary mechanisms of action: HA provides immediate lubrication and cartilage protection, while PRP creates a restorative and anti-inflammatory environment by releasing growth factors [26].
Safety and adverse effects:
The safety profile of both PRP and HA treatments has been evaluated as favorable. As summarized in Table 2, the adverse effects reported across all studies were limited, mild, and transient.
The most common adverse effect was temporary pain or swelling at the injection site, which typically resolved spontaneously within 24-72 hours. Large studies, including Chen et al. (2023) [18] and Khalid et al. (2024) [19], reported no serious or systemic treatment-related adverse events. Furthermore, a study on PRP+HA combination therapy showed that adding PRP to HA did not alter the safety profile, and its adverse effects were similar to those of the control group [26]. These findings generally indicate that intra-articular injections of PRP and HA are safe and acceptable interventions with low adverse event rates.
Discussion
This systematic review aimed to evaluate the efficacy and safety of PRP and HA, used as monotherapies or in combination, for the treatment of knee OA. The results indicated that both treatment methods led to significant improvements in patients’ clinical indices, including WOMAC, VAS, IKDC, EQ-VAS, and Tegner scores [27-29]. Overall, no significant difference was observed between PRP and HA in terms of pain relief or safety during long-term follow-up, consistent with previous studies [29].
However, subgroup and longitudinal analyses revealed that PRP, particularly LP-PRP formulations, improved total IKDC and WOMAC scores compared to HA and LR-PRP, suggesting that PRP may offer greater long-term functional benefits [30, 31]. These findings are also consistent with biological mechanisms, as PRP contains growth factors that stimulate chondrocyte proliferation, regulate collagenase activity, and promote synthesis of the extracellular matrix. In contrast, HA lacks such regenerative effects [27]. Furthermore, the lower retreatment rate in the PRP group at 24 months may be clinically relevant, even though no significant difference in overall effect duration was observed [32].
The efficacy of PRP is influenced by variables such as leukocyte concentration, preparation method, and number of injections. Laboratory studies have shown that leukocytes may activate catabolic and inflammatory pathways, which can reduce long-term effects, whereas LP-PRP mitigates these negative impacts while preserving growth factor activity [33]. Additionally, using a double-spin centrifugation method for PRP preparation increases platelet and growth factor concentration, thereby enhancing therapeutic efficacy [32]. However, differences in formulations and injection protocols led to variable clinical outcomes, underscoring the necessity for standardization in this field [27].
The combination of PRP and HA may have a synergistic effect; HA contributes through lubrication and mechanical protection, while PRP provides regenerative effects, together aiding in pain reduction and functional improvement. Meta-analyses and previous studies indicate that the PRP + HA combination leads to greater reductions in WOMAC scores and better functional outcomes compared to either treatment alone, especially at long-term follow-up [34, 35]. The mechanism of this synergy may involve regulation of inflammatory cytokines, such as interleukin-1 beta (IL-1β) and tumor necrosis factor (TNF)-α, activation of TGF-β signaling pathways, and enhanced cartilage repair via CD44 and TGF-beta type II receptor (βRII) [36].
Despite these positive results, the study has limitations. Variations in follow-up duration, PRP preparation methods, injection volume, and patient characteristics (age, KL grade, degree of cartilage degeneration) can lead to heterogeneity in the results [37]. Furthermore, the limited number of long-term RCTs and incomplete reporting of adverse events prevent definitive conclusions regarding the absolute superiority of one treatment over the other. Although PRP demonstrated better long-term functional outcomes, no significant differences were observed in pain relief or safety, necessitating further studies with standardized protocols, adequate sample sizes, and follow-up periods exceeding 24 months [38].
In summary, this study confirms the efficacy of both PRP and HA in reducing Knee OA symptoms and improving knee function. LP-PRP, either alone or combined with HA, may provide greater long-term functional benefits and a lower retreatment rate compared to HA or LR-PRP, although further research is essential to optimize PRP formulations and injection strategies. The findings of this study offer important clinical insights for selecting injectable therapies for patients with knee OA and emphasize that treatment decisions should be based on biological mechanisms and individual patient characteristics [37-39].
Conclusion
The present study demonstrated that both LR-PRP and HA improve pain, joint function, and the duration of effect in patients with knee OA. However, PRP, particularly its LP-PRP, showed a tendency toward reduced reinjection requirements and greater long-term functional improvement. Both treatments were safe and well-tolerated; however, PRP’s potential for achieving more sustained clinical effects suggests it may be a preferable option for long-term symptom management. Confirming these findings and optimizing treatment strategies requires large-scale, long-term clinical trials with standardized PRP protocols.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Omid Safaee; Methodology: Bushra Zareie; Validation, formal analysis, resources, and data curation: Ali Torkaman, Mohsen Fathi Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Chen D, Shen J, Zhao W, Wang T, Han L, Hamilton JL, et al. Osteoarthritis: Toward a comprehensive understanding of pathological mechanism. Bone Res. 2017; 5:16044. [DOI:10.1038/boneres.2016.44] [PMID]
- Han S. Osteoarthritis year in review 2022: Biology. Osteoarthritis Cartilage. 2022; 30(12):1575-82. [PMID]
- Demelash KM, Belay SA, Mulat H, Diriba T, Molla YD. Prevalence and associated factors of femoral shaft fractures among patients admitted with extremity fractures: Experience from the largest trauma center in Ethiopia. BMC Surg. 2026; 26(1):186. [DOI:10.1186/s12893-026-03574-z] [PMID]
- Bortoluzzi A, Furini F, Scirè CA. Osteoarthritis and its management - Epidemiology, nutritional aspects and environmental factors. Autoimmun Rev. 2018; 17(11):1097-104. [DOI:10.1016/j.autrev.2018.06.002] [PMID]
- Brandt MD, Malone JB, Kean TJ. Advances and challenges in the pursuit of disease-modifying osteoarthritis drugs: A review of 2010-2024 clinical trials. Biomedicines. 2025; 13(2):355. [DOI:10.3390/biomedicines13020355] [PMID]
- Allen KD, Thoma LM, Golightly YM. Epidemiology of osteoarthritis. Osteoarthritis Cartilage. 2022; 30(2):184-95. [DOI:10.1016/j.joca.2021.04.020] [PMID]
- Kloppenburg M, Berenbaum F. Osteoarthritis year in review 2019: Epidemiology and therapy. Osteoarthritis Cartilage. 2020; 28(3):242-8. [DOI:10.1016/j.joca.2020.01.002] [PMID]
- Peng Y, Yang L, Qi A, Zhang L, Xiong R, Chen G. Simulation-based learning combined with case and problem-based learning in the clinical education of joint surgery. J Surg Educ. 2023; 80(6):892-9. [DOI:10.1016/j.jsurg.2023.03.001] [PMID]
- Kang LJ, Yoon J, Rho JG, Han HS, Lee S, Oh YS, et al. Self-assembled hyaluronic acid nanoparticles for osteoarthritis treatment. Biomaterials. 2021; 275:120967. [DOI:10.1016/j.biomaterials.2021.120967] [PMID]
- Sato A, Kawabata H, Aizawa H, Tsujino T, Isobe K, Watanabe T, et al. Distribution and quantification of activated platelets in platelet-rich fibrin matrices. Platelets. 2022; 33(1):110-5. [DOI:10.1080/09537104.2020.1856359] [PMID]
- Han Y, Huang H, Pan J, Lin J, Zeng L, Liang G, et al. Meta-analysis comparing platelet-rich plasma vs hyaluronic acid injection in patients with knee osteoarthritis. Pain Med. 2019; 20(7):1418-29. [PMID]
- Andia I, Atilano L, Maffulli N. Moving toward targeting the right phenotype with the right platelet-rich plasma (PRP) formulation for knee osteoarthritis. Ther Adv Musculoskelet Dis. 2021; 13:1759720X211004336. [DOI:10.1177/1759720x211004336] [PMID]
- Kon E, Di Matteo B, Delgado D, Cole BJ, Dorotei A, Dragoo JL, et al. Platelet-rich plasma for the treatment of knee osteoarthritis: An expert opinion and proposal for a novel classification and coding system. Expert Opin Biol Ther. 2020; 20(12):1447-60. [DOI:10.1080/14712598.2020.1798925] [PMID]
- Bennell KL, Bayram C, Harrison C, Brand C, Buchbinder R, Haas R, et al. Trends in management of hip and knee osteoarthritis in general practice in Australia over an 11-year window: A nationwide cross-sectional survey. Lancet Reg Health West Pac. 2021; 12:100187. [DOI:10.1016/j.lanwpc.2021.100187] [PMID]
- Everts P, Onishi K, Jayaram P, Lana JF, Mautner K. Platelet-rich plasma: New performance understandings and therapeutic considerations in 2020. Int J Mol Sci. 2020; 21(20):7794. [DOI:10.3390/ijms21207794] [PMID]
- Belk JW, Houck DA, Littlefield CP, Kraeutler MJ, Potyk AG, Mei-Dan O, et al. Platelet-rich plasma versus hyaluronic acid for hip osteoarthritis yields similarly beneficial short-term clinical outcomes: A systematic review and meta-analysis of level I and II randomized controlled trials. Arthroscopy. 2022; 38(6):2035-46. [DOI:10.1016/j.arthro.2021.11.005] [PMID]
- Saturveithan C, Premganesh G, Fakhrizzaki S, Mahathir M, Karuna K, Rauf K, et al. Intra-articular hyaluronic acid (HA) and platelet rich plasma (PRP) injection versus Hyaluronic acid (HA) injection alone in patients with grade iii and iv knee osteoarthritis (OA): A retrospective study on functional outcome. Malays Orthop J. 2016; 10(2):35-40. [DOI:10.5704/moj.1607.007] [PMID]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. [DOI:10.1136/bmj.n71] [PMID]
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366:l4898. [DOI:10.1136/bmj.l4898] [PMID]
- Chen L, Jin S, Yao Y, He S, He J. Comparison of clinical efficiency between intra-articular injection of platelet-rich plasma and hyaluronic acid for osteoarthritis: A meta-analysis of randomized controlled trials. Ther Adv Musculoskelet Dis. 2023; 15:1759720X231157043. [DOI:10.1177/1759720x231157043] [PMID]
- Khalid S, Ali A, Deepak F, Zulfiqar MS, Malik LU, Fouzan Z, et al. Comparative effectiveness of intra-articular therapies in knee osteoarthritis: A meta-analysis comparing platelet-rich plasma (PRP) with other treatment modalities. Ann Med Surg (Lond). 2023; 86(1):361-72. [DOI:10.1097/ms9.0000000000001615] [PMID]
- Shoma FK, Rahman MM, Chowdhury ZR, Hassan MK, Hossain F, Rahman F, et al. Comparison of the effectiveness of platelet-rich plasma (PRP), hyaluronic acid and the combination of both in the treatment of mild and moderate osteoarthritis of the knee. J Dhaka Med Coll. 2019; 28(2):172-8. [Link]
- Guenoun D, Magalon J, de Torquemada I, Vandeville C, Sabatier F, Champsaur P, et al. Treatment of degenerative meniscal tear with intrameniscal injection of platelets rich plasma. Diagn Interv Imaging. 2020; 101(3):169-76. [DOI:10.1016/j.diii.2019.10.003] [PMID]
- Montañez-Heredia E, Irízar S, Huertas PJ, Otero E, Del Valle M, Prat I, et al. Intra-articular injections of platelet-rich plasma versus hyaluronic acid in the treatment of osteoarthritic knee pain: A randomized clinical trial in the context of the Spanish national health care system. Int J Mol Sci. 2016; 17(7):1064. [DOI:10.3390/ijms17071064] [PMID]
- Ivander G, Anggono Y. A comparison of intra-articular hyaluronic acid and platelet-rich plasma for knee osteoarthritis: A systematic review. Orthop Rev (Pavia). 2024; 16:94236. [PMID]
- Erdem Y, Gül D, Akpancar S. Comparison of intraarticular injections of hyaluronic acid versus dextrose applied with periarticular prolotherapy in the treatment of recreational athletes with knee osteoarthritis. Turk J Sports Med. 2020; 55(1):6-13. [Link]
- Raeissadat SA, Ghazi Hosseini P, Bahrami MH, Salman Roghani R, Fathi M, Gharooee Ahangar A, et al. The comparison effects of intra-articular injection of platelet rich Plasma (PRP), plasma rich in growth factor (PRGF), hyaluronic acid (HA), and ozone in knee osteoarthritis; a one year randomized clinical trial. BMC Musculoskelet Disord. 2021; 22(1):134. [DOI:10.1186/s12891-021-04017-x] [PMID]
- Kirschner JS, Cheng J, Creighton A, Santiago K, Hurwitz N, Dundas M, et al. Efficacy of ultrasound-guided glenohumeral joint injections of leukocyte-poor platelet-rich plasma versus hyaluronic acid in the treatment of glenohumeral osteoarthritis: A randomized, double-blind controlled trial. Clin J Sport Med. 2022; 32(6):558-66. [DOI:10.1097/jsm.0000000000001029] [PMID]
- Mariani E, Canella V, Cattini L, Kon E, Marcacci M, Di Matteo B, et al. Leukocyte-rich platelet-rich plasma injections do not up-modulate intra-articular proinflammatory cytokines in the osteoarthritic knee. Plos One. 2016; 11(6):e0156137. [DOI:10.1371/journal.pone.0156137] [PMID]
- Say F, Gurler D, Yener K, Bulbul M, Malkoc M. Platelet-rich plasma injection is more effective than hyaluronic acid in the treatment of knee osteoarthritis. Acta Chir Orthop Traumatol Cech. 2013; 80(4):278-83. [PMID]
- Bennell KL, Hunter DJ, Paterson KL. Platelet-rich plasma for the management of hip and knee osteoarthritis. Curr Rheumatol Rep. 2017; 19(5):24. [DOI:10.1007/s11926-017-0652-x] [PMID]
- Hsueh MF, Zhang X, Wellman SS, Bolognesi MP, Kraus VB. Synergistic roles of macrophages and neutrophils in osteoarthritis progression. Arthritis Rheumatol. 2021; 73(1):89-99. [DOI:10.1002/art.41486] [PMID]
- Sundman EA, Cole BJ, Fortier LA. Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am J Sports Med. 2011; 39(10):2135-40. [DOI:10.1177/0363546511417792] [PMID]
- Laver L, Marom N, Dnyanesh L, Mei-Dan O, Espregueira-Mendes J, Gobbi A. PRP for degenerative cartilage disease: A systematic review of clinical studies. Cartilage. 2017; 8(4):341-64. [DOI:10.1177/1947603516670709] [PMID]
- Hesari R, Keshvarinia M, Kabiri M, Rad I, Parivar K, Hoseinpoor H, et al. Combination of low intensity electromagnetic field with chondrogenic agent induces chondrogenesis in mesenchymal stem cells with minimal hypertrophic side effects. Electromagn Biol Med. 2020; 39(2):154-65. [DOI:10.1080/15368378.2020.1737809] [PMID]
- Shen L, Yuan T, Chen S, Xie X, Zhang C. The temporal effect of platelet-rich plasma on pain and physical function in the treatment of knee osteoarthritis: Systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res. 2017; 12(1):16. [DOI:10.1186/s13018-017-0521-3] [PMID]
- Raeissadat SA, Rayegani SM, Hassanabadi H, Fathi M, Ghorbani E, Babaee M, et al. Knee osteoarthritis injection choices: Platelet- rich plasma (prp) versus hyaluronic acid (A one-year randomized clinical trial). Clin Med Insights Arthritis Musculoskelet Disord. 2015; 8:1-8. [DOI:10.4137/cmamd.s17894] [PMID]
- Singh H, Knapik DM, Polce EM, Eikani CK, Bjornstad AH, Gursoy S, et al. Relative efficacy of intra-articular injections in the treatment of knee osteoarthritis: A systematic review and network meta-analysis. Am J Sports Med. 2021; 50(11):3140-8. [DOI:10.1177/03635465211029659] [PMID]
- Chouhan DK, Dhillon MS, Patel S, Bansal T, Bhatia A, Kanwat H. Multiple platelet-rich plasma injections versus single platelet-rich plasma injection in early osteoarthritis of the knee: An experimental study in a Guinea pig model of early knee osteoarthritis. Am J Sports Med. 2019; 47(10):2300-7. [PMID]
Type of Study: Review Paper |
Subject:
Knee surgery
Received: 2025/02/2 | Accepted: 2025/04/21 | Published: 2025/11/1
Received: 2025/02/2 | Accepted: 2025/04/21 | Published: 2025/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
